

From statistical significance to clinical relevance: A simple algorithm to integrate brain natriuretic peptide and the Seattle Heart Failure Model for risk stratification in heart failure
- PMID: 27021278
- PMCID: PMC4917454
- DOI: 10.1016/j.healun.2016.01.016
From statistical significance to clinical relevance: A simple algorithm to integrate brain natriuretic peptide and the Seattle Heart Failure Model for risk stratification in heart failure
Abstract
Background: Heart failure (HF) guidelines recommend brain natriuretic peptide (BNP) and multivariable risk scores, such as the Seattle Heart Failure Model (SHFM), to predict risk in HF with reduced ejection fraction (HFrEF). A practical way to integrate information from these 2 prognostic tools is lacking. We sought to establish a SHFM+BNP risk-stratification algorithm.
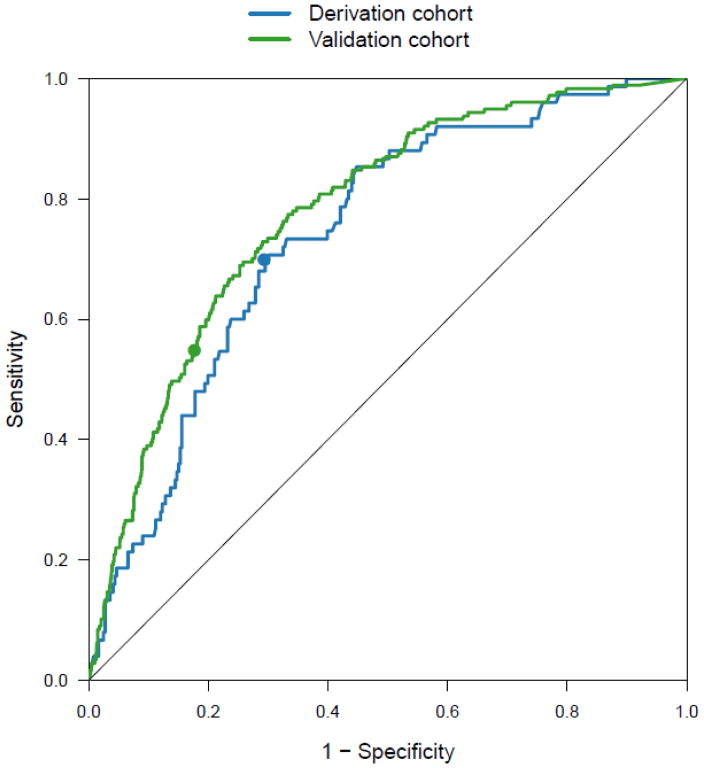
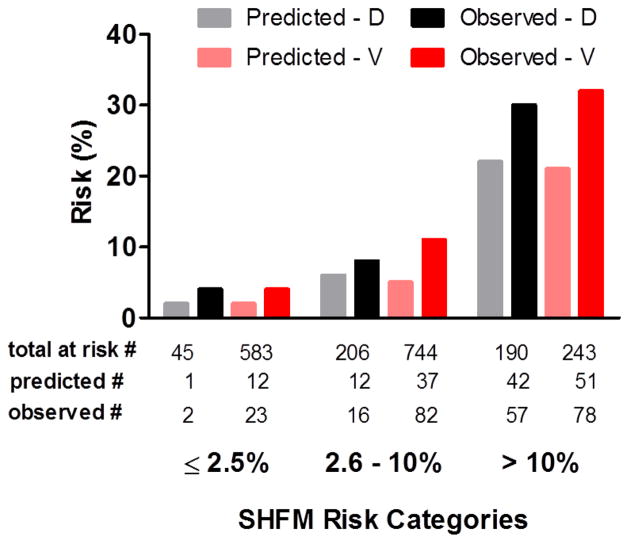
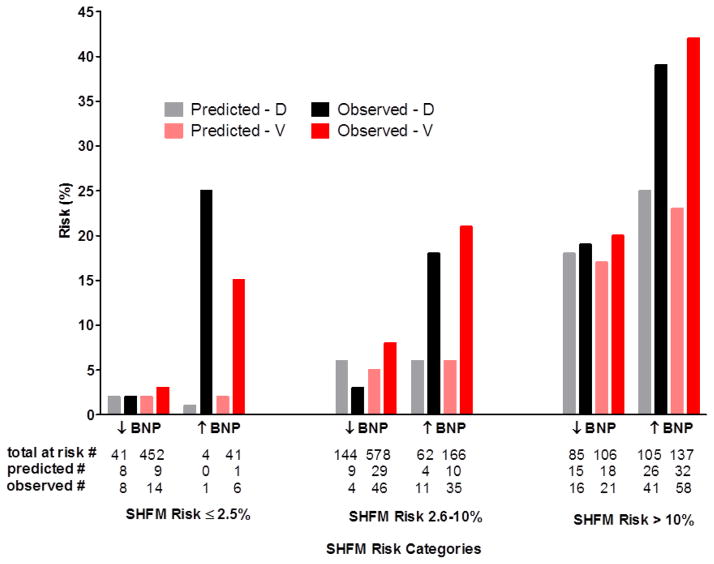
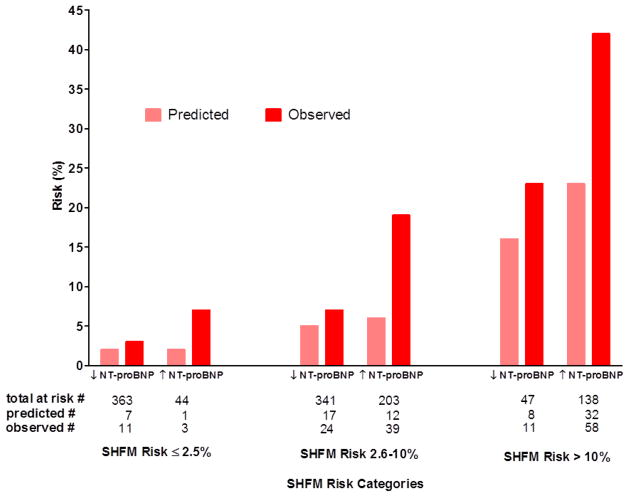
Methods: The retrospective derivation cohort included consecutive patients with HFrEF at the Mayo Clinic. One-year outcome (death, transplantation or ventricular assist device) was assessed. The SHFM+BNP algorithm was derived by stratifying patients within SHFM-predicted risk categories (≤2.5%, 2.6% to ≤10%, >10%) according to BNP above or below 700 pg/ml and comparing SHFM-predicted and observed event rates within each SHFM+BNP category. The algorithm was validated in a prospective, multicenter HFrEF registry (Penn HF Study).
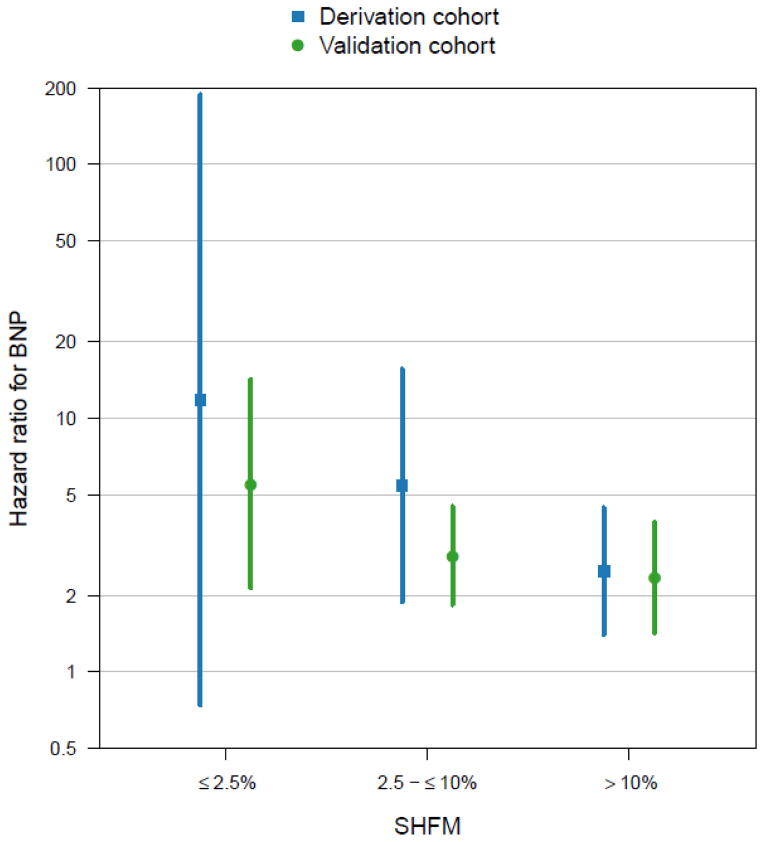
Results: Derivation (n = 441; 1-year event rate 17%) and validation (n = 1,513; 1-year event rate 12%) cohorts differed with the former being older and more likely ischemic with worse symptoms, lower EF, worse renal function and higher BNP and SHFM scores. In both cohorts, across the 3 SHFM-predicted risk strata, a BNP >700 pg/ml consistently identified patients with approximately 3-fold the risk that the SHFM would have otherwise estimated, regardless of stage of HF, intensity and duration of HF therapy and comorbidities. Conversely, the SHFM was appropriately calibrated in patients with a BNP <700 pg/ml.
Conclusion: The simple SHFM+BNP algorithm displays stable performance across diverse HFrEF cohorts and may enhance risk stratification to enable appropriate decision-making regarding HF therapeutic or palliative strategies.
Keywords: Seattle Heart Failure Model; biomarkers; heart failure; natriuretic peptides; prognosis; risk stratification.
Copyright © 2016 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Risk scores and biomarkers in heart failure: A journey to predictive accuracy and clinical utility.J Heart Lung Transplant. 2016 Jun;35(6):711-3. doi: 10.1016/j.healun.2016.04.003. Epub 2016 May 6. J Heart Lung Transplant. 2016. PMID: 27235269 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–239. - PubMed
-
- Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation. 2006;113:1424–33. - PubMed
-
- Gorodeski EZ, Chu EC, Chow CH, Levy WC, Hsich E, Starling RC. Application of the Seattle Heart Failure Model in ambulatory patients presented to an advanced heart failure therapeutics committee. Circ Heart Fail. 2010;3:706–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
