

Distal biceps ruptures: open and endoscopic techniques
- PMID: 27021282
- PMCID: PMC4896873
- DOI: 10.1007/s12178-016-9330-2
Distal biceps ruptures: open and endoscopic techniques
Abstract
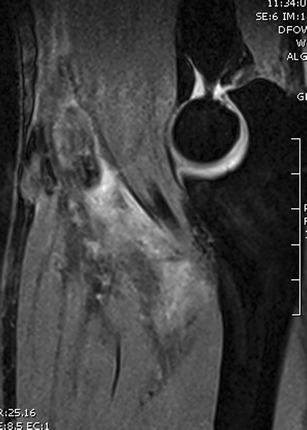
Distal biceps tendon ruptures are relatively rare. Patients are usually middle-aged men involved in heavy labor. Patients usually present with the history of a pop and a proximal migration of the biceps muscle belly. Clinical exam should be sufficient to diagnose a complete rupture. Several specific tests have been described. Ultrasound scanning or MRI can help confirm the diagnosis. Radiographs are not needed to diagnose distal biceps tendon rupture but may show typical findings. Imaging, more specifically the flexion-abduction-supination (FABS) view MRI, is particularly helpful in the case of a partial rupture or chronic rupture of the distal biceps tendon. Results of surgical reinsertion of the distal biceps have been shown to be superior to conservative treatment. Different techniques and approaches have been described with specific advantages and disadvantages. Primary repair of the tendon is preferred. If this is no longer possible in chronic tears, an augmentation can be done using tendon graft. Results of surgical treatment are good in the vast majority of patients. Reruptures are rare but minor complications are common. Major complications may include posterior interosseous nerve palsy or radioulnar synostosis, but the risk of these complications may be decreased by meticulous attention to detail during surgery.
Keywords: Avulsion; Biceps endoscopy; Biceps tendon; Double incision; Rupture; Single incision.
Figures











References
-
- Safran MR, Graham SM. Distal biceps tendon ruptures: incidence, demographics, and the effect of smoking. Clin Orthop Relat Res. 2002;404:275–83. - PubMed
-
- Kelly MP, Perkinson SG, Ablove RH, Tueting JL. Distal biceps tendon ruptures: an epidemiological analysis using a large population database. Am J Sports Med. 2015;43(8):2012–7. - PubMed
-
- Seiler JG, 3rd, Parker LM, Chamberland PD, Sherbourne GM, Carpenter WA. The distal biceps tendon. Two potential mechanisms involved in its rupture: arterial supply and mechanical impingement. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons [et al]. 1995;4(3):149-56. - PubMed
-
- Eames MH, Bain GI, Fogg QA, van Riet RP. Distal biceps tendon anatomy: a cadaveric study. J Bone Joint Surg Am. 2007;89(5):1044–9. - PubMed
-
- Pacha Vicente D, Forcada Calvet P, Carrera Burgaya A, Llusa PM. Innervation of biceps brachii and brachialis: anatomical and surgical approach. Clin Anat. 2005;18(3):186–94. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
