

Helicobacter pylori eradication therapy for functional dyspepsia: Systematic review and meta-analysis
- PMID: 27022230
- PMCID: PMC4806206
- DOI: 10.3748/wjg.v22.i12.3486
Helicobacter pylori eradication therapy for functional dyspepsia: Systematic review and meta-analysis
Abstract
Aim: To evaluate whether Helicobacter pylori (H. pylori) eradication therapy benefits patients with functional dyspepsia (FD).
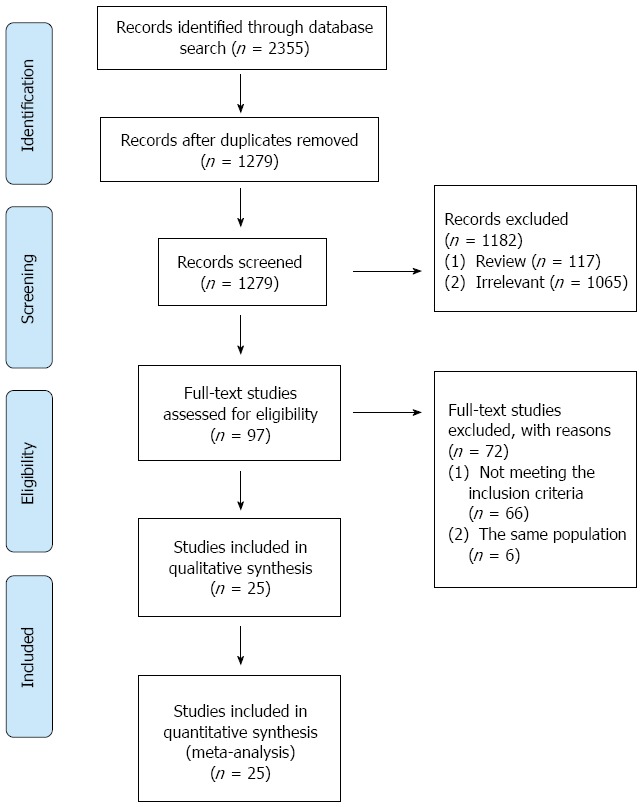
Methods: Randomized controlled trials (RCTs) investigating the efficacy and safety of H. pylori eradication therapy for patients with functional dyspepsia published in English (up to May 2015) were identified by searching PubMed, EMBASE, and The Cochrane Library. Pooled estimates were measured using the fixed or random effect model. Overall effect was expressed as a pooled risk ratio (RR) or a standard mean difference (SMD). All data were analyzed with Review Manager 5.3 and Stata 12.0.
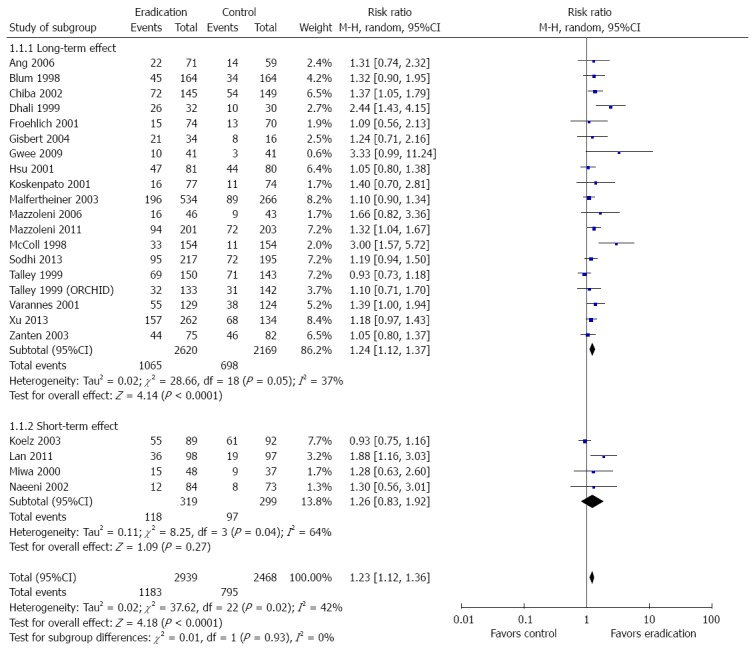
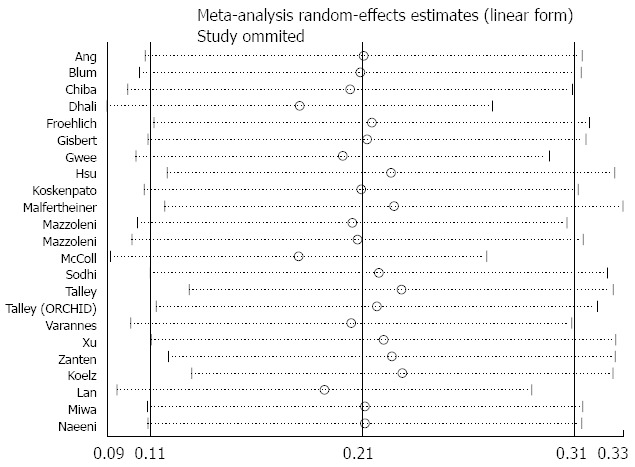
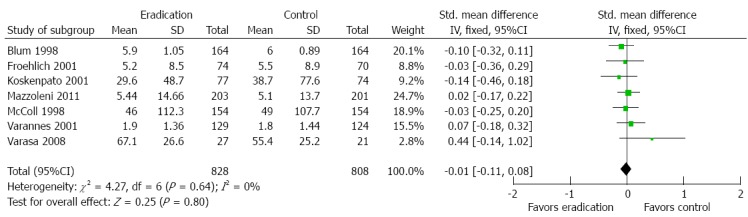
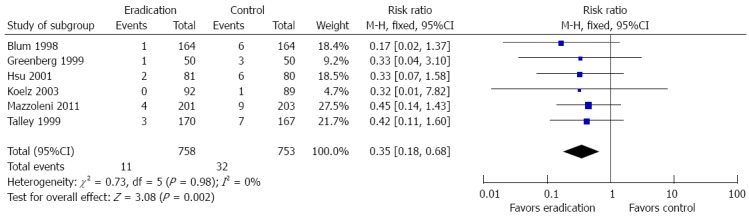
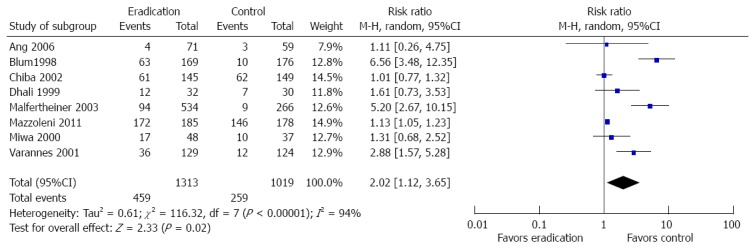
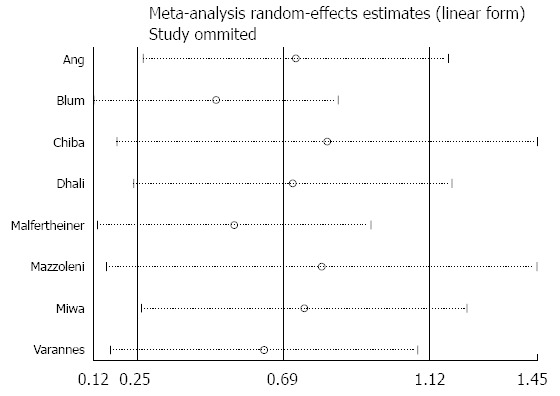
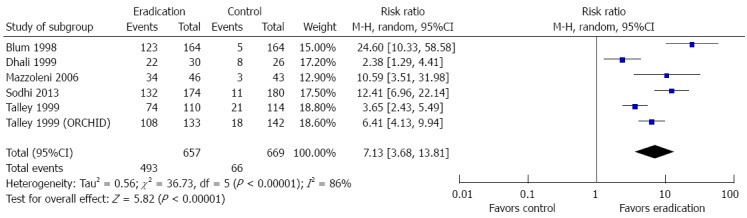
Results: This systematic review included 25 RCTs with a total of 5555 patients with FD. Twenty-three of these studies were used to evaluate the benefits of H. pylori eradication therapy for symptom improvement; the pooled RR was 1.23 (95%CI: 1.12-1.36, P < 0.0001). H. pylori eradication therapy demonstrated symptom improvement during long-term follow-up at ≥ 1 year (RR = 1.24; 95%CI: 1.12-1.37, P < 0.0001) but not during short-term follow-up at < 1 year (RR = 1.26; 95%CI: 0.83-1.92, P = 0.27). Seven studies showed no benefit of H. pylori eradication therapy on quality of life with an SMD of -0.01 (95%CI: -0.11 to 0.08, P = 0.80). Six studies demonstrated that H. pylori eradication therapy reduced the development of peptic ulcer disease compared to no eradication therapy (RR = 0.35; 95%CI: 0.18-0.68, P = 0.002). Eight studies showed that H. pylori eradication therapy increased the likelihood of treatment-related side effects compared to no eradication therapy (RR = 2.02; 95%CI: 1.12-3.65, P = 0.02). Ten studies demonstrated that patients who received H. pylori eradication therapy were more likely to obtain histologic resolution of chronic gastritis compared to those who did not receive eradication therapy (RR = 7.13; 95%CI: 3.68-13.81, P < 0.00001).
Conclusion: The decision to eradicate H. pylori in patients with functional dyspepsia requires individual assessment.
Keywords: Functional dyspepsia; Helicobacter pylori eradication; Meta-analysis; Peptic ulceration; Quality of life; Symptom improvement.
Figures
References
-
- Ford AC, Marwaha A, Sood R, Moayyedi P. Global prevalence of, and risk factors for, uninvestigated dyspepsia: a meta-analysis. Gut. 2015;64:1049–1057. - PubMed
-
- Zhao Y, Zou D, Wang R, Ma X, Yan X, Man X, Gao L, Fang J, Yan H, Kang X, et al. Dyspepsia and irritable bowel syndrome in China: a population-based endoscopy study of prevalence and impact. Aliment Pharmacol Ther. 2010;32:562–572. - PubMed
-
- Li Y, Nie Y, Sha W, Su H. The link between psychosocial factors and functional dyspepsia: an epidemiological study. Chin Med J (Engl) 2002;115:1082–1084. - PubMed
-
- Tack J, Talley NJ, Camilleri M, Holtmann G, Hu P, Malagelada JR, Stanghellini V. Functional gastroduodenal disorders. Gastroenterology. 2006;130:1466–1479. - PubMed
-
- Samsom M, Verhagen MA, vanBerge Henegouwen GP, Smout AJ. Abnormal clearance of exogenous acid and increased acid sensitivity of the proximal duodenum in dyspeptic patients. Gastroenterology. 1999;116:515–520. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
