

Impact of Comorbidities on Mortality in Patients with Idiopathic Pulmonary Fibrosis
- PMID: 27023440
- PMCID: PMC4811578
- DOI: 10.1371/journal.pone.0151425
Impact of Comorbidities on Mortality in Patients with Idiopathic Pulmonary Fibrosis
Abstract
Introduction: Comorbidities significantly influence the clinical course of idiopathic pulmonary fibrosis (IPF). However, their prognostic impact is not fully understood. We therefore aimed to determine the impact of comorbidities, as individual and as whole, on survival in IPF.
Methods: The database of a tertiary referral centre for interstitial lung diseases was reviewed for comorbidities, their treatments, their frequency and survival in IPF patients.
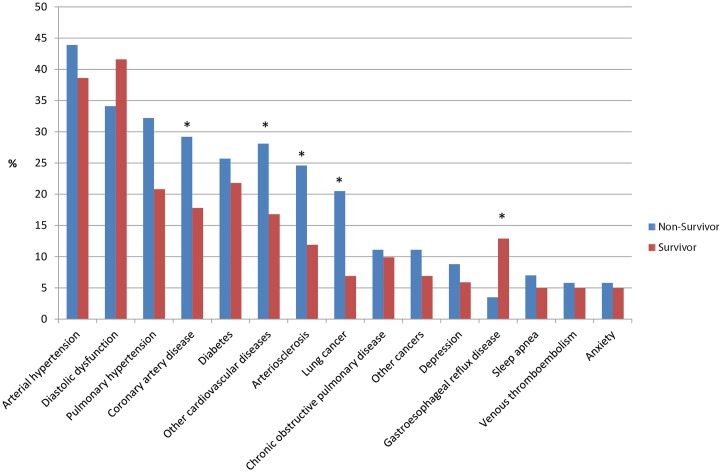
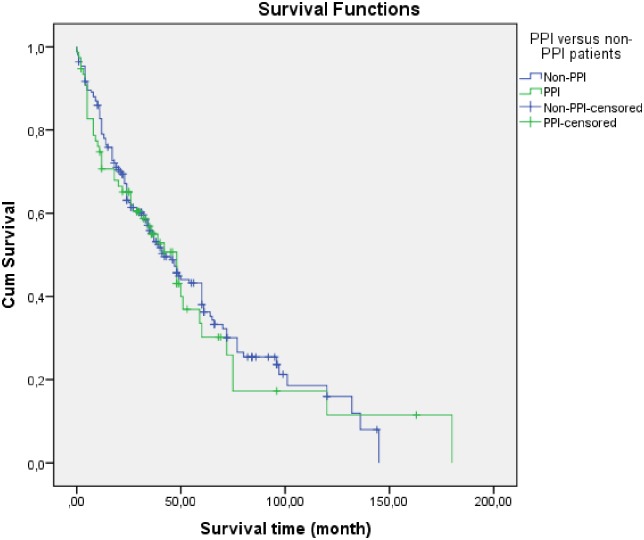
Results: 272 patients were identified of which 12% had no, 58% 1-3 and 30% 4-7 comorbidities, mainly cardiovascular, pulmonary and oncologic comorbidities. Median survival according to the frequency of comorbidities differed significantly with 66 months for patients without comorbidities, 48 months when 1-3 comorbidities were reported and 35 months when 4-7 comorbidities were prevalent (p = 0.004). A multivariate Cox proportional hazard analyses identified other cardiac diseases and lung cancer as significant predictors of death, gastro-oesophageal reflux disease (GERD) and diastolic dysfunction had a significant positive impact on survival. A significant impact of comorbidities associated therapies on survival was not discovered. This included the use of proton pump inhibitors at baseline, which was not associated with a survival benefit (p = 0.718). We also established a predictive tool for highly prevalent comorbidities, termed IPF comorbidome which demonstrates a new relationship of IPF and comorbidities.
Conclusion: Comorbidities are frequent in IPF patients. Some comorbidities, especially lung cancer, mainly influence survival in IPF, while others such as GERD may inherit a more favourable effect. Moreover, their cumulative incidence impacts survival.
Conflict of interest statement
Figures




References
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK et al. ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011. March 15;183(6):788–824. 10.1164/rccm.2009-040GL - DOI - PMC - PubMed
-
- Lettieri CJ, Nathan SD, Barnett SD, Ahmad S, Shorr AF. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2006. March;129(3):746–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
