

CHA2DS2-VASc-HS score in non-ST elevation acute coronary syndrome patients: assessment of coronary artery disease severity and complexity and comparison to other scoring systems in the prediction of in-hospital major adverse cardiovascular events
- PMID: 27025198
- PMCID: PMC5324933
- DOI: 10.14744/AnatolJCardiol.2015.6593
CHA2DS2-VASc-HS score in non-ST elevation acute coronary syndrome patients: assessment of coronary artery disease severity and complexity and comparison to other scoring systems in the prediction of in-hospital major adverse cardiovascular events
Abstract
Objective: We recently described the CHA2DS2-VASc-HS score as a novel predictor of coronary artery disease (CAD) severity in stable CAD patients. We aimed to assess the accuracy of the CHA2DS2-VASc-HS score in the determination of CAD severity and complexity and its availability in the risk stratification of in-hospital major adverse cardiovascular events (MACE) in non-ST elevation acute coronary syndrome (NSTE-ACS) patients.
Methods: We prospectively analyzed the clinical and angiographic data of consecutive NSTE-ACS patients in our clinic. Patients were classified into three tertiles according to their SYNTAX score (SS): tertile 1 had an SS of 0-22; tertile 2 had an SS of 23-32; and tertile 3 had an SS of >32. There were no specific exclusion criteria except for previous coronary artery bypass grafting (CABG) because SS was validated for only native coronary arteries for this study. We used the following analyses: χ2 or Fisher's exact tests, one-way analysis of variance or Kruskal-Wallis tests, Pearson's or Spearman's tests, the receiver operating characteristics (ROC) curve analysis, the area under the curve (AUC) or C-statistic, and pairwise comparisons of the ROC curves.
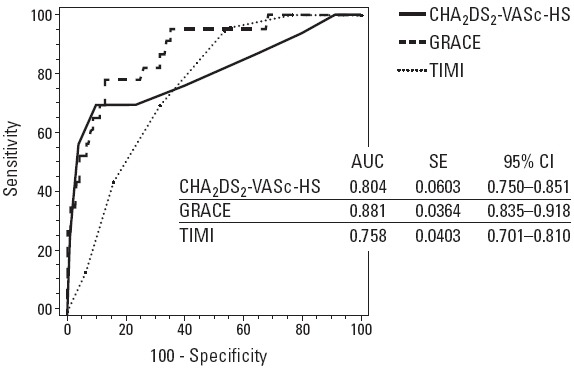
Results: A total of 252 patients were enrolled. There were 131 patients in tertile 1, 79 in tertile 2, and 42 in tertile 3. The number of diseased vessels was correlated with the Global Registry for Acute Coronary Events (GRACE) (p<0.001), Thrombolysis in Myocardial Infarction (TIMI) (p<0.001), and CHA2DS2-VASc-HS (p<0.001) scores. In the ROC curve analyses, the cut-off value of the CHA2DS2-VASc-HS score in the prediction of in-hospital MACE was >5 with a sensitivity of 69.6% and specificity of 90.3% (AUC: 0.804, 95%: CI 0.750-0.851, p<0.001). We also compared the diagnostic accuracy of the CHA2DS2-VASc-HS score with the TIMI and GRACE risk scores in the determination of the in-hospital MACE and found no differences.
Conclusion: The CHA2DS2-VASc-HS score was positively correlated with the severity and complexity of CAD. We also found that CHA2DS2-VASc-HS was comparable with other risk scores for the risk stratification of the in-hospital MACE of NSTE-ACS patients. Therefore, it may play an important role as a predictive model of NSTE-ACS patients in clinical practice.
Conflict of interest statement
Figures
Similar articles
-
Coronary artery disease severity and risk stratification of patients with non ST-elevation acute coronary syndrome using CHA2DS2-VASc-HSF score.BMC Cardiovasc Disord. 2024 May 21;24(1):263. doi: 10.1186/s12872-024-03929-5. BMC Cardiovasc Disord. 2024. PMID: 38773382 Free PMC article.
-
Prediction of coronary artery disease severity using CHADS2 and CHA2DS2-VASc scores and a newly defined CHA2DS2-VASc-HS score.Am J Cardiol. 2014 Mar 15;113(6):950-6. doi: 10.1016/j.amjcard.2013.11.056. Epub 2013 Dec 25. Am J Cardiol. 2014. PMID: 24444782
-
Usefulness of the CHA2DS2-VASc Score to Predict Adverse Outcomes in Acute Coronary Syndrome Patients Without Atrial Fibrillation Undergoing Percutaneous Coronary Intervention.Am J Cardiol. 2019 Aug 15;124(4):476-484. doi: 10.1016/j.amjcard.2019.05.036. Epub 2019 May 29. Am J Cardiol. 2019. PMID: 31235063
-
The Management and Prognostic Factors of Acute Coronary Syndrome: Evidence from the Taiwan Acute Coronary Syndrome Full Spectrum Registry.Acta Cardiol Sin. 2017 Jul;33(4):329-338. doi: 10.6515/acs20161205a. Acta Cardiol Sin. 2017. PMID: 29033503 Free PMC article. Review.
-
Prehospital risk assessment in patients suspected of non-ST-segment elevation acute coronary syndrome: a systematic review and meta-analysis.BMJ Open. 2022 Apr 5;12(4):e057305. doi: 10.1136/bmjopen-2021-057305. BMJ Open. 2022. PMID: 35383078 Free PMC article.
Cited by
-
Association of GRACE Risk Score with Coronary Artery Disease Complexity in Patients with Acute Coronary Syndrome.J Clin Med. 2021 May 20;10(10):2210. doi: 10.3390/jcm10102210. J Clin Med. 2021. PMID: 34065227 Free PMC article.
-
Usefulness of the CHADS2 and R2CHADS2 scores for prognostic stratification in patients with coronary artery disease.Clin Interv Aging. 2018 Apr 5;13:565-571. doi: 10.2147/CIA.S156208. eCollection 2018. Clin Interv Aging. 2018. PMID: 29670341 Free PMC article.
-
Prognostic value of CHA2DS2-VASc score for the long-term cardiovascular events after coronary artery bypass grafting.Turk Gogus Kalp Damar Cerrahisi Derg. 2023 Oct 19;31(4):479-488. doi: 10.5606/tgkdc.dergisi.2023.24964.. eCollection 2023 Oct. Turk Gogus Kalp Damar Cerrahisi Derg. 2023. PMID: 38076003 Free PMC article.
-
Predictive value of CHA2DS2-VASc and CHA2DS2-VASc-HS scores for failed reperfusion after thrombolytic therapy in patients with ST-segment elevation myocardial infarction.Cardiol J. 2019;26(2):169-175. doi: 10.5603/CJ.a2018.0017. Epub 2018 Mar 7. Cardiol J. 2019. PMID: 29512096 Free PMC article.
-
Utilization of NaF-PET/CT in assessing global cardiovascular calcification using CHADS2 and CHADS2-VASc scoring systems in high risk individuals for cardiovascular disease.Am J Nucl Med Mol Imaging. 2020 Dec 15;10(6):293-300. eCollection 2020. Am J Nucl Med Mol Imaging. 2020. PMID: 33329931 Free PMC article.
References
-
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al. European Association for Cardiovascular Prevention & Rehabilitation (EACPR);ESC Committee for Practice Guidelines (CPG). European Guidelines on cardiovascular disease prevention in clinical practice (version. 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Eur Heart J. 2012;33:1635–701. - PubMed
-
- Wright RS, Anderson JL, Adams CD, Bridges CR, Casey DE, Jr, Ettinger SM, et al. 2011 ACCF/AHA focused update of the Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction (updating the 2007 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American College of Emergency Physicians, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57:1920–59. - PubMed
-
- Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, et al. Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2010;31:2501–55. - PubMed
-
- Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, Papuchis G, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–42. - PubMed
-
- Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6- month postdischarge death in an international registry. JAMA. 2004;291:2727–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
