

Empirical tuberculosis therapy versus isoniazid in adult outpatients with advanced HIV initiating antiretroviral therapy (REMEMBER): a multicountry open-label randomised controlled trial
- PMID: 27025337
- PMCID: PMC4931281
- DOI: 10.1016/S0140-6736(16)00546-8
Empirical tuberculosis therapy versus isoniazid in adult outpatients with advanced HIV initiating antiretroviral therapy (REMEMBER): a multicountry open-label randomised controlled trial
Abstract
Background: Mortality within the first 6 months after initiating antiretroviral therapy is common in resource-limited settings and is often due to tuberculosis in patients with advanced HIV disease. Isoniazid preventive therapy is recommended in HIV-positive adults, but subclinical tuberculosis can be difficult to diagnose. We aimed to assess whether empirical tuberculosis treatment would reduce early mortality compared with isoniazid preventive therapy in high-burden settings.
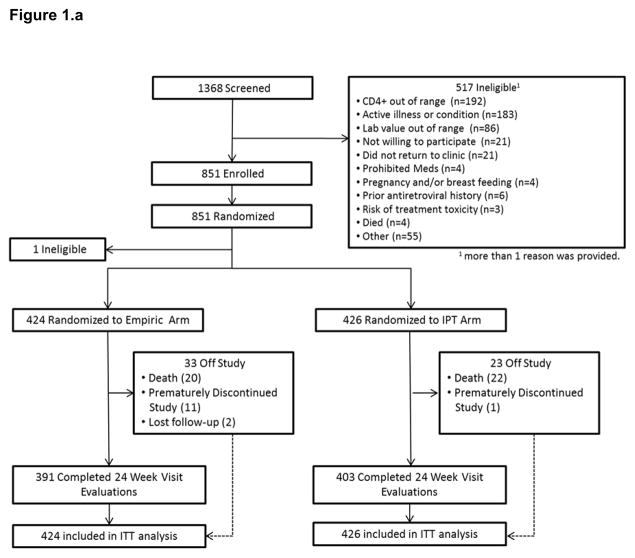
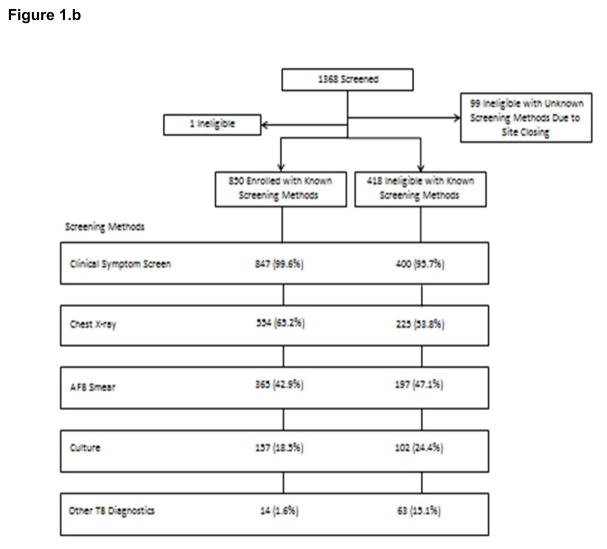
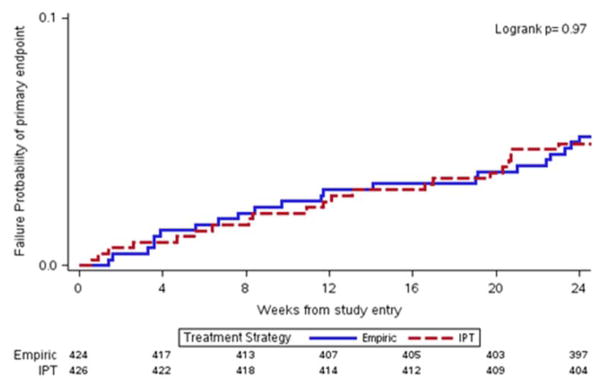
Methods: We did a multicountry open-label randomised clinical trial comparing empirical tuberculosis therapy with isoniazid preventive therapy in HIV-positive outpatients initiating antiretroviral therapy with CD4 cell counts of less than 50 cells per μL. Participants were recruited from 18 outpatient research clinics in ten countries (Malawi, South Africa, Haiti, Kenya, Zambia, India, Brazil, Zimbabwe, Peru, and Uganda). Individuals were screened for tuberculosis using a symptom screen, locally available diagnostics, and the GeneXpert MTB/RIF assay when available before inclusion. Study candidates with confirmed or suspected tuberculosis were excluded. Inclusion criteria were liver function tests 2·5 times the upper limit of normal or less, a creatinine clearance of at least 30 mL/min, and a Karnofsky score of at least 30. Participants were randomly assigned (1:1) to either the empirical group (antiretroviral therapy and empirical tuberculosis therapy) or the isoniazid preventive therapy group (antiretroviral therapy and isoniazid preventive therapy). The primary endpoint was survival (death or unknown status) at 24 weeks after randomisation assessed in the intention-to-treat population. Kaplan-Meier estimates of the primary endpoint across groups were compared by the z-test. All participants were included in the safety analysis of antiretroviral therapy and tuberculosis treatment. This trial is registered with ClinicalTrials.gov, number NCT01380080.
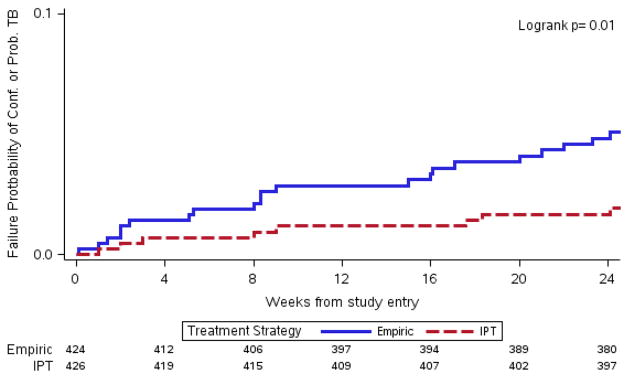
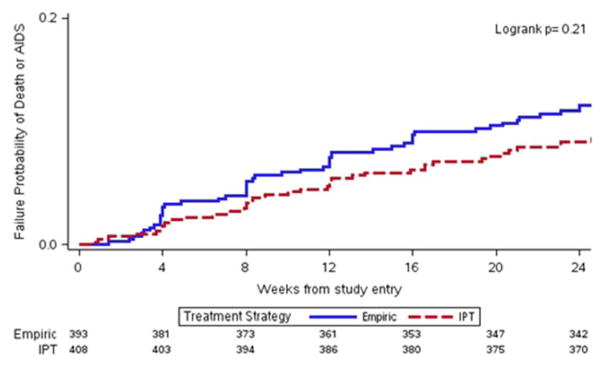
Findings: Between Oct 31, 2011, and June 9, 2014, we enrolled 850 participants. Of these, we randomly assigned 424 to receive empirical tuberculosis therapy and 426 to the isoniazid preventive therapy group. The median CD4 cell count at baseline was 18 cells per μL (IQR 9-32). At week 24, 22 (5%) participants from each group died or were of unknown status (95% CI 3·5-7·8) for empirical group and for isoniazid preventive therapy (95% CI 3·4-7·8); absolute risk difference of -0·06% (95% CI -3·05 to 2·94). Grade 3 or 4 signs or symptoms occurred in 50 (12%) participants in the empirical group and 46 (11%) participants in the isoniazid preventive therapy group. Grade 3 or 4 laboratory abnormalities occurred in 99 (23%) participants in the empirical group and 97 (23%) participants in the isoniazid preventive therapy group.
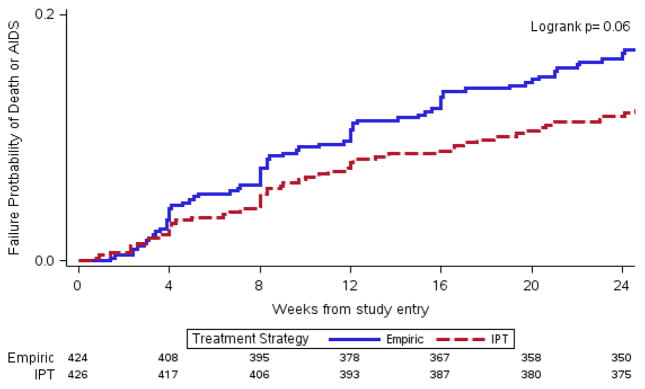
Interpretation: Empirical tuberculosis therapy did not reduce mortality at 24 weeks compared with isoniazid preventive therapy in outpatient adults with advanced HIV disease initiating antiretroviral therapy. The low mortality rate of the trial supports implementation of systematic tuberculosis screening and isoniazid preventive therapy in outpatients with advanced HIV disease.
Funding: National Institutes of Allergy and Infectious Diseases through the AIDS Clinical Trials Group.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Why are people living with HIV still dying of tuberculosis?Lancet. 2016 Mar 19;387(10024):1141-3. doi: 10.1016/S0140-6736(16)00699-1. Lancet. 2016. PMID: 27025319 No abstract available.
References
-
- UNAIDS. How AIDS changed everything: MDG 6: 15 YEARS, 15 LESSONS OF HOPE FROM THE AIDS ESPONSE. [accessed July 14 2015 2015];Fact Sheet. 2015 http://www.unaids.org/sites/default/files/media_asset/20150714_FS_MDG6_R....
-
- Lawn SD, Badri M, Wood R. Tuberculosis among HIV-infected patients receiving HAART: long term incidence and risk factors in a South African cohort. AIDS. 2005;19(18):2109–16. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069423/AI/NIAID NIH HHS/United States
- UM1 AI069476/AI/NIAID NIH HHS/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI069469/AI/NIAID NIH HHS/United States
- UM1 AI069518/AI/NIAID NIH HHS/United States
- UM1 AI069453/AI/NIAID NIH HHS/United States
- UM1 AI069463/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1 AI108568/AI/NIAID NIH HHS/United States
- HH-SN272200800014C/HH/HHS/United States
- UM1 AI069436/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
