

The Natural History of Flare-Ups in Fibrodysplasia Ossificans Progressiva (FOP): A Comprehensive Global Assessment
- PMID: 27025942
- PMCID: PMC4829946
- DOI: 10.1002/jbmr.2728
The Natural History of Flare-Ups in Fibrodysplasia Ossificans Progressiva (FOP): A Comprehensive Global Assessment
Abstract
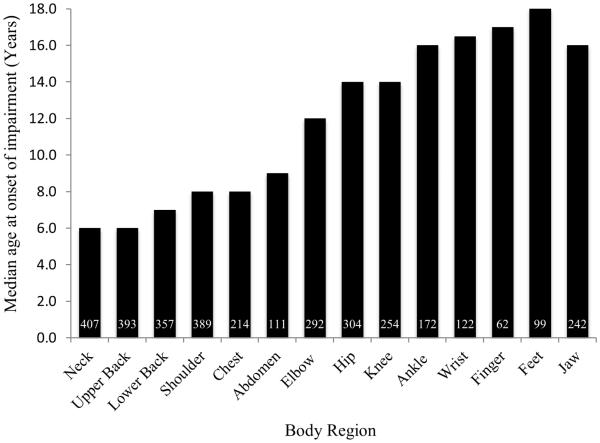
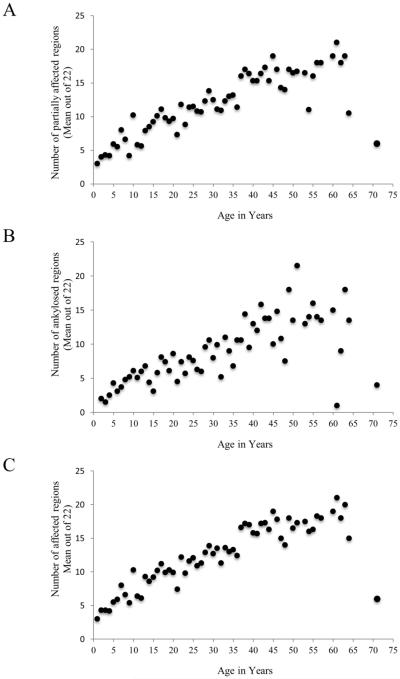
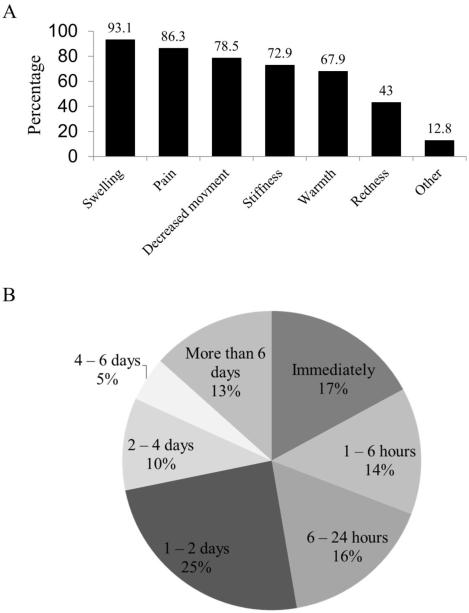
Fibrodysplasia ossificans progressiva (FOP) leads to disabling heterotopic ossification (HO) from episodic flare-ups. However, the natural history of FOP flare-ups is poorly understood. A 78-question survey on FOP flare-ups, translated into 15 languages, was sent to 685 classically-affected patients in 45 countries (six continents). Five hundred patients or knowledgeable informants responded (73%; 44% males, 56% females; ages: 1 to 71 years; median: 23 years). The most common presenting symptoms of flare-ups were swelling (93%), pain (86%), or decreased mobility (79%). Seventy-one percent experienced a flare-up within the preceding 12 months (52% spontaneous; 48% trauma-related). Twenty-five percent of those who had received an intramuscular injection reported an immediate flare-up at the injection site, 84% of whom developed HO. Axial flare-ups most frequently involved the back (41.6%), neck (26.4%), or jaw (19.4%). Flare-ups occurred more frequently in the upper limbs before 8 years of age, but more frequently in the lower limbs thereafter. Appendicular flare-ups occurred more frequently at proximal than at distal sites without preferential sidedness. Seventy percent of patients reported functional loss from a flare-up. Thirty-two percent reported complete resolution of at least one flare-up and 12% without any functional loss (mostly in the head or back). The most disabling flare-ups occurred at the shoulders or hips. Surprisingly, 47% reported progression of FOP without obvious flare-ups. Worldwide, 198 treatments were reported; anti-inflammatory agents were most common. Seventy-five percent used short-term glucocorticoids as a treatment for flare-ups at appendicular sites. Fifty-five percent reported that glucocorticoids improved symptoms occasionally whereas 31% reported that they always did. Only 12% reported complete resolution of a flare-up with glucocorticoids. Forty-three percent reported rebound symptoms within 1 to 7 days after completing a course of glucocorticoids. This study is the first comprehensive global assessment of FOP flare-ups and establishes a critical foundation for the design and evaluation of future clinical trials.
Keywords: CLINICAL TRIALS; EPIDEMIOLOGY; FIBRODYSPLASIA OSSIFICANS PROGRESSIVA; FOP.
© 2015 American Society for Bone and Mineral Research.
Figures
References
-
- Shore EM, Xu M, Feldman GJ, Fenstermacher DA, Cho TJ, Choi IH, Connor JM, Delai P, Glaser DL, LeMerrer M, Morhart R, Rogers JG, Smith R, Triffitt JT, Urtizberea JA, Zasloff M, Brown MA, Kaplan FS. A recurrent mutation in the BMP type I receptor ACVR1 causes inherited and sporadic fibrodysplasia ossificans progressiva. Nat Genet. 2006 May;38(5):525–7. - PubMed
-
- Cohen RB, Hahn GV, Tabas JA, Peeper J, Levitz CL, Sando A, Sando N, Zasloff M, Kaplan FS. The natural history of heterotopic ossification in patients who have fibrodysplasia ossificans progressiva. A study of forty-four patients. J Bone Joint Surg Am. 1993 Feb;75(2):215–9. - PubMed
