

An in vitro analysis of medial structures and a medial soft tissue reconstruction in a constrained condylar total knee arthroplasty
- PMID: 27026029
- PMCID: PMC5522503
- DOI: 10.1007/s00167-016-4087-0
An in vitro analysis of medial structures and a medial soft tissue reconstruction in a constrained condylar total knee arthroplasty
Erratum in
-
Erratum to: An in vitro analysis of medial structures and a medial soft tissue reconstruction in a constrained condylar total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2017 Aug;25(8):2656. doi: 10.1007/s00167-017-4583-x. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 28681087 Free PMC article. No abstract available.
Abstract
Purpose: The aim of this study was to quantify the medial soft tissue contributions to stability following constrained condylar (CC) total knee arthroplasty (TKA) and determine whether a medial reconstruction could restore stability to a soft tissue-deficient, CC-TKA knee.
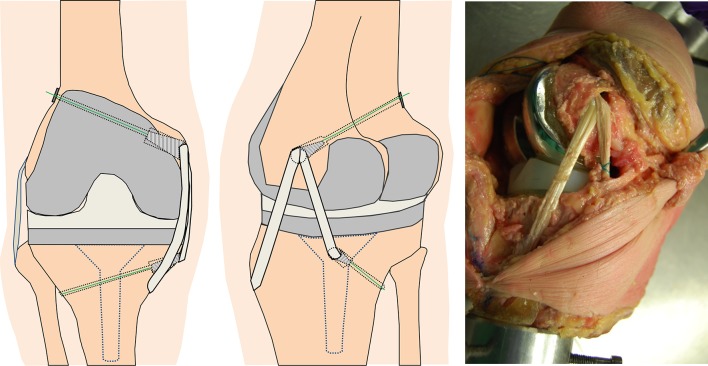
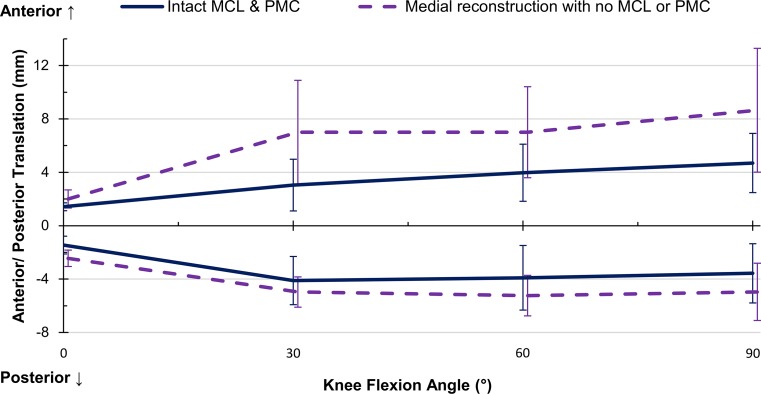
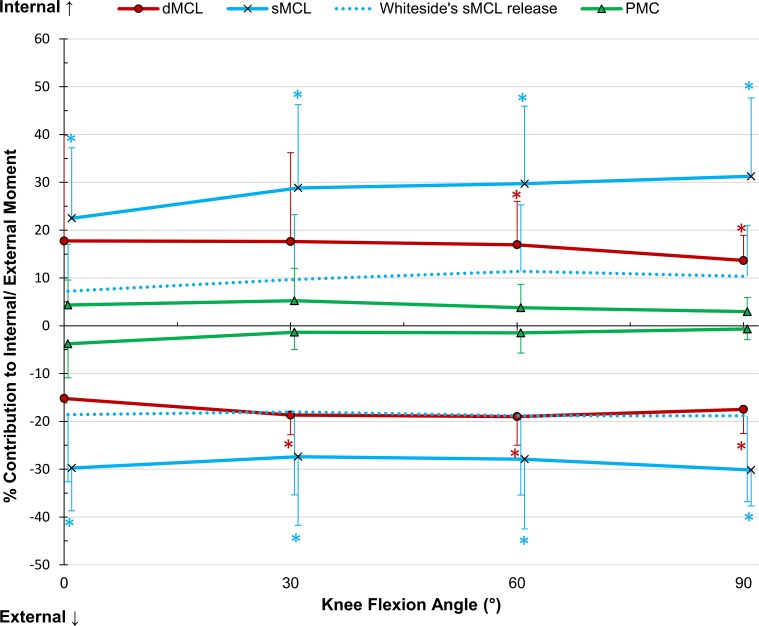
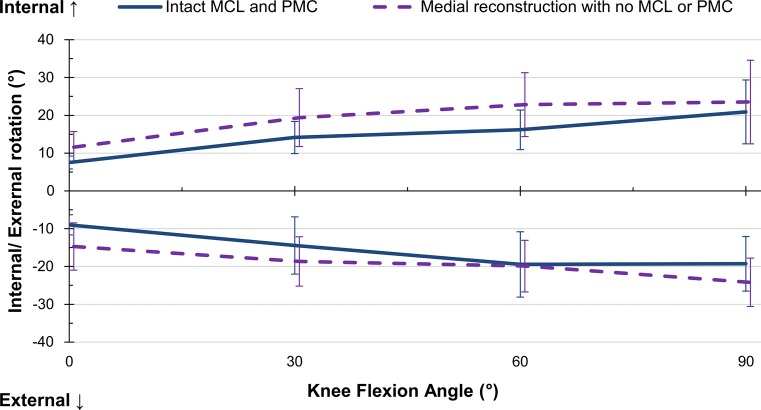
Methods: Eight cadaveric knees were mounted in a robotic system and tested at 0°, 30°, 60°, and 90° of flexion with ±50 N anterior-posterior force, ±8 Nm varus-valgus, and ±5 Nm internal-external torque. The deep and superficial medial collateral ligaments (dMCL, sMCL) and posteromedial capsule (PMC) were transected and their relative contributions to stabilising the applied loads were quantified. After complete medial soft tissue transection, a reconstruction using a semitendinosus tendon graft was performed, and the effect on kinematic behaviour under equivocal conditions was measured.
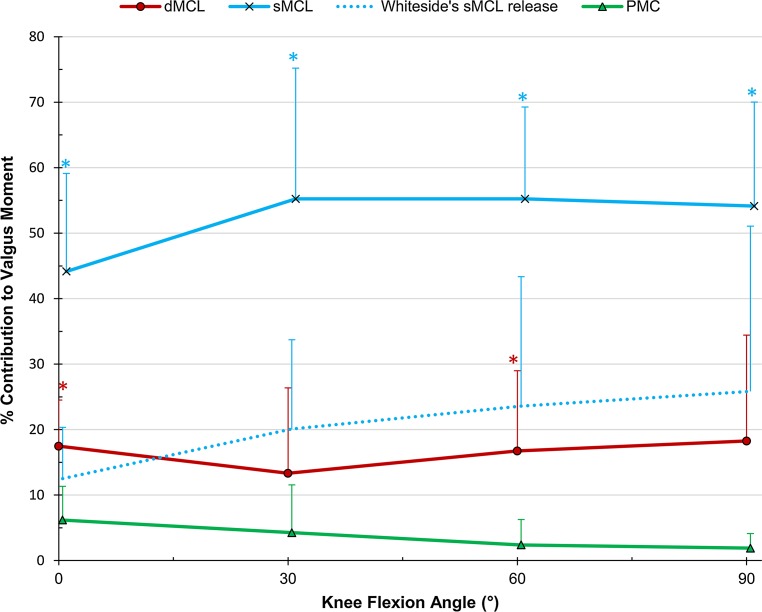
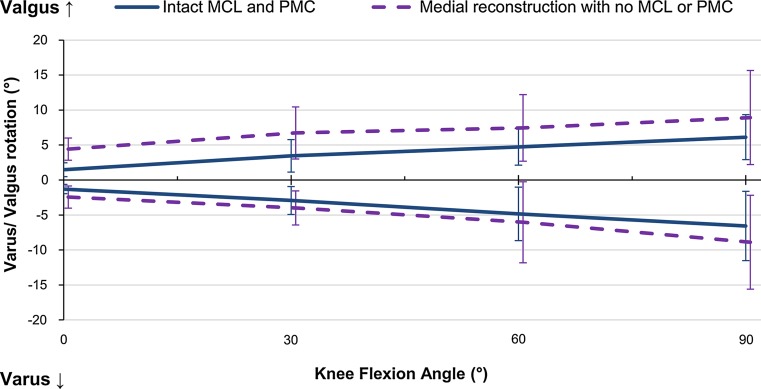
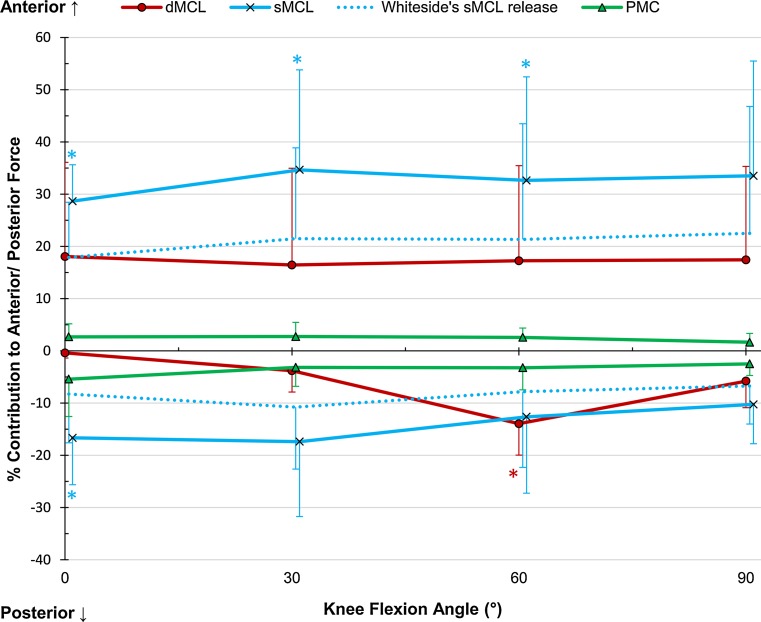
Results: In the CC-TKA knee, the sMCL was the major medial restraint in anterior drawer, internal-external, and valgus rotation. No significant differences were found between the rotational laxities of the reconstructed knee to the pre-deficient state for the arc of motion examined. The relative contribution of the reconstruction was higher in valgus rotation at 60° than the sMCL; otherwise, the contribution of the reconstruction was similar to that of the sMCL.
Conclusion: There is contention whether a CC-TKA can function with medial deficiency or more constraint is required. This work has shown that a CC-TKA may not provide enough stability with an absent sMCL. However, in such cases, combining the CC-TKA with a medial soft tissue reconstruction may be considered as an alternative to a hinged implant.
Keywords: Constrained implant; Knee replacement; Laxity; Medial collateral ligament; Reconstruction; Soft tissue deficiency; Stability; Total knee arthroplasty.
Figures
References
-
- Amis AA, Scammell BE. Biomechanics of intra-articular and extra-articular reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br. 1993;75:812–817. - PubMed
-
- Athwal KK, El Daou H, Kittl C, Davies AJ, Deehan DJ, Amis AA. The superficial medial collateral ligament is the primary medial restraint to knee laxity after cruciate-retaining or posterior-stabilised total knee arthroplasty: effects of implant type and partial release. Knee Surg Sports Traumatol Arthrosc. 2015 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
