

Review of evolving etiologies, implications and treatment strategies for the superior vena cava syndrome
- PMID: 27026923
- PMCID: PMC4771672
- DOI: 10.1186/s40064-016-1900-7
Review of evolving etiologies, implications and treatment strategies for the superior vena cava syndrome
Abstract
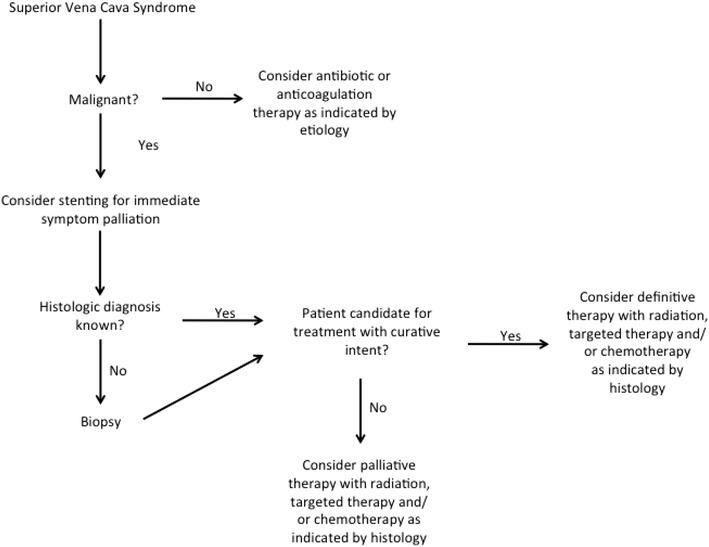
Superior vena cava syndrome (SVCS) is a relatively common sequela of mediastinal malignancies and may cause significant patient distress. SVCS is a medical emergency if associated with laryngeal or cerebral edema. The etiologies and management of SVCS have evolved over time. Non-malignant SVCS is typically caused by infectious etiologies or by thrombus in the superior vena cava and can be managed with antibiotics or anti-coagulation therapy, respectively. Radiation therapy (RT) has long been a mainstay of treatment of malignant SVCS. Chemotherapy has also been used to manage SVCS. In the past 20 years, percutaneous stenting of the superior vena cava has emerged as a viable option for SVCS symptom palliation. RT and chemotherapy are still the only modalities that can provide curative treatment for underlying malignant etiologies of SVCS. The first experiences with treating SVCS with RT were reported in the 1970's, and several advances in RT delivery have subsequently occurred. Hypo-fractionated RT has the potential to be a more convenient therapy for patients and may provide equal or superior control of underlying malignancies. RT may be combined with stenting and/or chemotherapy to provide both immediate symptom palliation and long-term disease control. Clinicians should tailor therapy on a case-by-case basis. Multi-disciplinary care will maximize treatment expediency and efficacy.
Keywords: Hypo-fractionation; Multi-modality therapy; Stenting; Superior vena cava syndrome (SVC syndrome, SVCS); Thoracic malignancies.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
