

Short-Term Effects of Phenobarbitone on Electrographic Seizures in Neonates
- PMID: 27027306
- PMCID: PMC5079066
- DOI: 10.1159/000443782
Short-Term Effects of Phenobarbitone on Electrographic Seizures in Neonates
Abstract
Background: Phenobarbitone is the most common first-line anti-seizure drug and is effective in approximately 50% of all neonatal seizures.
Objective: To describe the response of electrographic seizures to the administration of intravenous phenobarbitone in neonates using seizure burden analysis techniques.
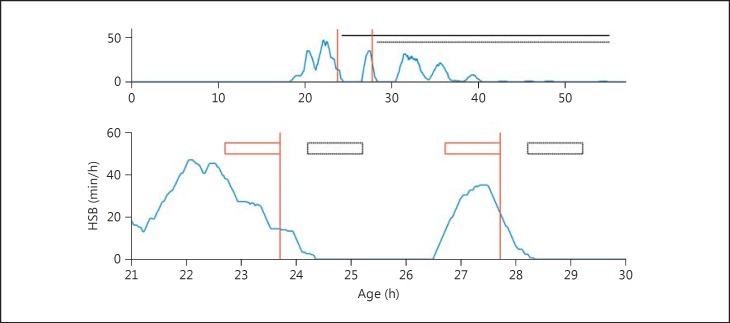
Methods: Multi-channel conventional EEG, reviewed by experts, was used to determine the electrographic seizure burden in hourly epochs. The maximum seizure burden evaluated 1 h before each phenobarbitone dose (T-1) was compared to seizure burden in periods of increasing duration after each phenobarbitone dose had been administered (T+1, T+2 to seizure offset). Differences were analysed using linear mixed models and summarized as means and 95% CI.
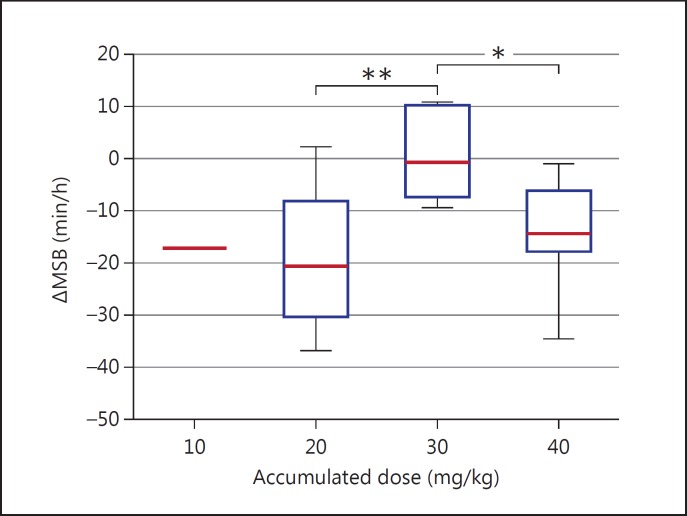
Results: Nineteen neonates had electrographic seizures and met the inclusion criteria for the study. Thirty-one doses were studied. The maximum seizure burden was significantly reduced 1 h after the administration of phenobarbitone (T+1) [-14.0 min/h (95% CI: -19.6, -8.5); p < 0.001]. The percentage reduction was 74% (IQR: 36-100). This reduction was temporary and not significant within 4 h of administrating phenobarbitone. Subgroup analysis showed that only phenobarbitone doses at 20 mg/kg resulted in a significant reduction in the maximum seizure burden from T-1 to T+1 (p = 0.002).
Conclusions: Phenobarbitone significantly reduced seizures within 1 h of administration as assessed with continuous multi-channel EEG monitoring in neonates. The reduction was not permanent and seizures were likely to return within 4 h of treatment.
© 2016 S. Karger AG, Basel.
Figures
Similar articles
-
Phenobarbitone versus phenytoin for treatment of neonatal seizures: an open-label randomized controlled trial.Indian Pediatr. 2013 Aug;50(8):753-7. doi: 10.1007/s13312-013-0218-6. Epub 2012 Dec 5. Indian Pediatr. 2013. PMID: 23502660 Clinical Trial.
-
Effect of Withholding Phenobarbitone Maintenance in Neonatal Seizures: A Randomized Controlled Trial.Indian Pediatr. 2016 Dec 15;53(12):1069-1073. Epub 2016 Nov 5. Indian Pediatr. 2016. PMID: 27889710 Clinical Trial.
-
Phenobarbitone, neonatal seizures, and video-EEG.Arch Dis Child Fetal Neonatal Ed. 2002 May;86(3):F165-70. doi: 10.1136/fn.86.3.f165. Arch Dis Child Fetal Neonatal Ed. 2002. PMID: 11978746 Free PMC article.
-
Efficacy and Safety of Phenobarbitone as First-Line Treatment for Neonatal Seizure: A Systematic Review and Meta-Analysis.J Trop Pediatr. 2021 Jan 29;67(1):fmab008. doi: 10.1093/tropej/fmab008. J Trop Pediatr. 2021. PMID: 33598701
-
Detection of electrographic seizures with continuous EEG monitoring in critically ill patients.Neurology. 2004 May 25;62(10):1743-8. doi: 10.1212/01.wnl.0000125184.88797.62. Neurology. 2004. PMID: 15159471 Review.
Cited by
-
Prognostic value of neonatal EEG following therapeutic hypothermia in survivors of hypoxic-ischemic encephalopathy.Clin Neurophysiol. 2021 Sep;132(9):2091-2100. doi: 10.1016/j.clinph.2021.05.031. Epub 2021 Jul 1. Clin Neurophysiol. 2021. PMID: 34284244 Free PMC article.
-
Treatment Trials for Neonatal Seizures: The Effect of Design on Sample Size.PLoS One. 2016 Nov 8;11(11):e0165693. doi: 10.1371/journal.pone.0165693. eCollection 2016. PLoS One. 2016. PMID: 27824913 Free PMC article.
-
Role of NKCC1 and KCC2 in Epilepsy: From Expression to Function.Front Neurol. 2020 Jan 17;10:1407. doi: 10.3389/fneur.2019.01407. eCollection 2019. Front Neurol. 2020. PMID: 32010056 Free PMC article. Review.
-
Treating the symptom or treating the disease in neonatal seizures: a systematic review of the literature.Ital J Pediatr. 2021 Apr 7;47(1):85. doi: 10.1186/s13052-021-01027-2. Ital J Pediatr. 2021. PMID: 33827647 Free PMC article.
-
Defining neonatal status epilepticus: A scoping review from the ILAE neonatal task force.Epilepsia Open. 2025 Feb;10(1):40-54. doi: 10.1002/epi4.13090. Epub 2024 Nov 14. Epilepsia Open. 2025. PMID: 39540265 Free PMC article.
References
-
- Thibeault-Eybalin MP, Lortie A, Carmant L. Neonatal seizures: do they damage the brain? Pediatr Neurol. 2009;40:175–180. - PubMed
-
- WHO: Guidelines on Neonatal Seizures. Geneva: World Health Organization; 2011. - PubMed
-
- Painter MJ, Scher MS, Stein AD, Armatti S, Wang Z, Gardiner JC, et al. Phenobarbital compared with phenytoin for the treatment of neonatal seizures. N Engl J Med. 1999;341:485–489. - PubMed
-
- Pressler RM, Mangum B. Newly emerging therapies for neonatal seizures. Semin Fetal Neonatal Med. 2013;18:216–223. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
