

Insulin resistance: a new consequence of altered carotid body chemoreflex?
- PMID: 27027507
- PMCID: PMC5199745
- DOI: 10.1113/JP271684
Insulin resistance: a new consequence of altered carotid body chemoreflex?
Abstract
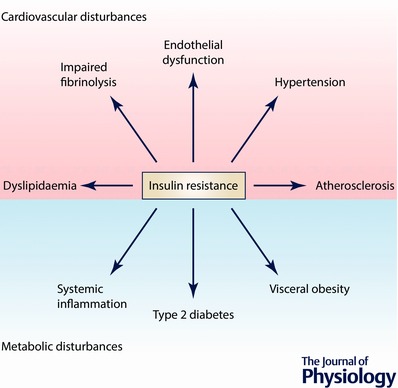
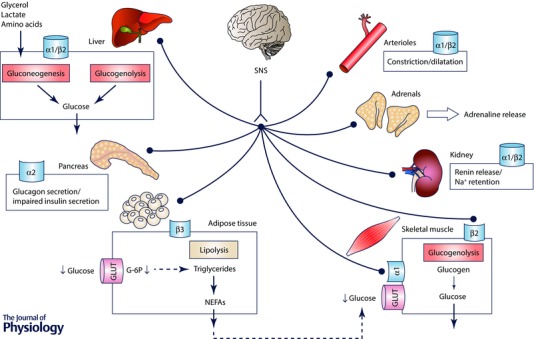
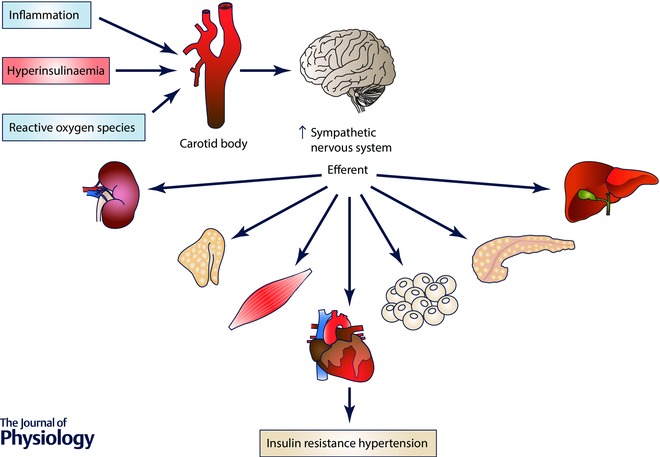
Metabolic diseases affect millions of individuals across the world and represent a group of chronic diseases of very high prevalence and relatively low therapeutic success, making them suitable candidates for pathophysiological studies. The sympathetic nervous system (SNS) contributes to the regulation of energy balance and energy expenditure both in physiological and pathological states. For instance, drugs that stimulate sympathetic activity decrease food intake, increase resting metabolic rate and increase the thermogenic response to food, while pharmacological blockade of the SNS has opposite effects. Likewise, dysmetabolic features such as insulin resistance, dyslipidaemia and obesity are characterized by a basal overactivation of the SNS. Recently, a new line of research linking the SNS to metabolic diseases has emerged with the report that the carotid bodies (CBs) are involved in the development of insulin resistance. The CBs are arterial chemoreceptors that classically sense changes in arterial blood O2 , CO2 and pH levels and whose activity is known to be increased in rodent models of insulin resistance. We have shown that selective bilateral resection of the nerve of the CB, the carotid sinus nerve (CSN), totally prevents diet-induced insulin resistance, hyperglycaemia, dyslipidaemia, hypertension and sympathoadrenal overactivity. These results imply that the beneficial effects of CSN resection on insulin action and glucoregulation are modulated by target-related efferent sympathetic nerves through a reflex that is initiated in the CBs. It also highlights modulation of CB activity as a putative future therapeutic intervention for metabolic diseases.
© 2016 The Authors. The Journal of Physiology © 2016 The Physiological Society.
Figures
Similar articles
-
Exploring the Mediators that Promote Carotid Body Dysfunction in Type 2 Diabetes and Obesity Related Syndromes.Int J Mol Sci. 2020 Aug 3;21(15):5545. doi: 10.3390/ijms21155545. Int J Mol Sci. 2020. PMID: 32756352 Free PMC article. Review.
-
Carotid body, insulin, and metabolic diseases: unraveling the links.Front Physiol. 2014 Oct 29;5:418. doi: 10.3389/fphys.2014.00418. eCollection 2014. Front Physiol. 2014. PMID: 25400585 Free PMC article. Review.
-
Carotid body denervation prevents the development of insulin resistance and hypertension induced by hypercaloric diets.Diabetes. 2013 Aug;62(8):2905-16. doi: 10.2337/db12-1463. Epub 2013 Mar 25. Diabetes. 2013. PMID: 23530003 Free PMC article.
-
High fat diet blunts the effects of leptin on ventilation and on carotid body activity.J Physiol. 2018 Aug;596(15):3187-3199. doi: 10.1113/JP275362. Epub 2018 Jan 15. J Physiol. 2018. PMID: 29271068 Free PMC article.
-
Functional abolition of carotid body activity restores insulin action and glucose homeostasis in rats: key roles for visceral adipose tissue and the liver.Diabetologia. 2017 Jan;60(1):158-168. doi: 10.1007/s00125-016-4133-y. Epub 2016 Oct 16. Diabetologia. 2017. PMID: 27744526
Cited by
-
Abnormal cardiovascular control during exercise: Role of insulin resistance in the brain.Auton Neurosci. 2025 Apr;258:103239. doi: 10.1016/j.autneu.2025.103239. Epub 2025 Jan 19. Auton Neurosci. 2025. PMID: 39874739 Free PMC article. Review.
-
Glucose, insulin, and the carotid body chemoreceptors in humans.Physiol Genomics. 2018 Jul 1;50(7):504-509. doi: 10.1152/physiolgenomics.00032.2018. Epub 2018 Apr 13. Physiol Genomics. 2018. PMID: 29652633 Free PMC article. Review.
-
Immunity and the carotid body: implications for metabolic diseases.Bioelectron Med. 2020 Dec 23;6(1):24. doi: 10.1186/s42234-020-00061-5. Bioelectron Med. 2020. PMID: 33353562 Free PMC article. Review.
-
Reversal of Diabesity Through Modulating Sympathetic Inputs to Adipose Tissue Following Carotid Body Resection.Acta Physiol (Oxf). 2025 Jul;241(7):e70074. doi: 10.1111/apha.70074. Acta Physiol (Oxf). 2025. PMID: 40552544 Free PMC article.
-
Bioelectronic modulation of carotid sinus nerve to treat type 2 diabetes: current knowledge and future perspectives.Front Neurosci. 2024 Apr 5;18:1378473. doi: 10.3389/fnins.2024.1378473. eCollection 2024. Front Neurosci. 2024. PMID: 38646610 Free PMC article. Review.
References
-
- Aguilar M, Bhuket T, Torres S, Liu B & Wong RJ (2015). Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 313, 1973–1974. - PubMed
-
- Arcaro G, Cretti A, Balzano S, Lechi A, Muggeo M, Bonora E & Bonadonna RC (2002). Insulin causes endothelial dysfunction in humans: sites and mechanisms. Circulation 105, 576–582. - PubMed
-
- Ardilouze JL, Sotorník R, Dennis LA, Fielding BA, Frayn KN & Karpe F (2012). Failure to increase postprandial blood flow in subcutaneous adipose tissue is associated with tissue resistance to adrenergic stimulation. Diabetes Metab 38, 27–33. - PubMed
-
- Arner P (2001). Genetic variance and lipolysis regulation: implications for obesity. Ann Med 33, 542–546. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical