

Fluid Overload Is Associated With Late Poor Outcomes in Neonates Following Cardiac Surgery
- PMID: 27028790
- PMCID: PMC4856556
- DOI: 10.1097/PCC.0000000000000715
Fluid Overload Is Associated With Late Poor Outcomes in Neonates Following Cardiac Surgery
Abstract
Objectives: Acute kidney injury is a severe complication of cardiac surgery associated with increased morbidity and mortality; yet, acute kidney injury classification for neonates remains challenging. We characterized patterns of postoperative fluid overload as a surrogate marker for acute kidney injury and as a risk factor of poor postoperative outcomes in neonates undergoing cardiac surgery.
Design: Retrospective cohort study.
Setting: Single, congenital heart center destination program.
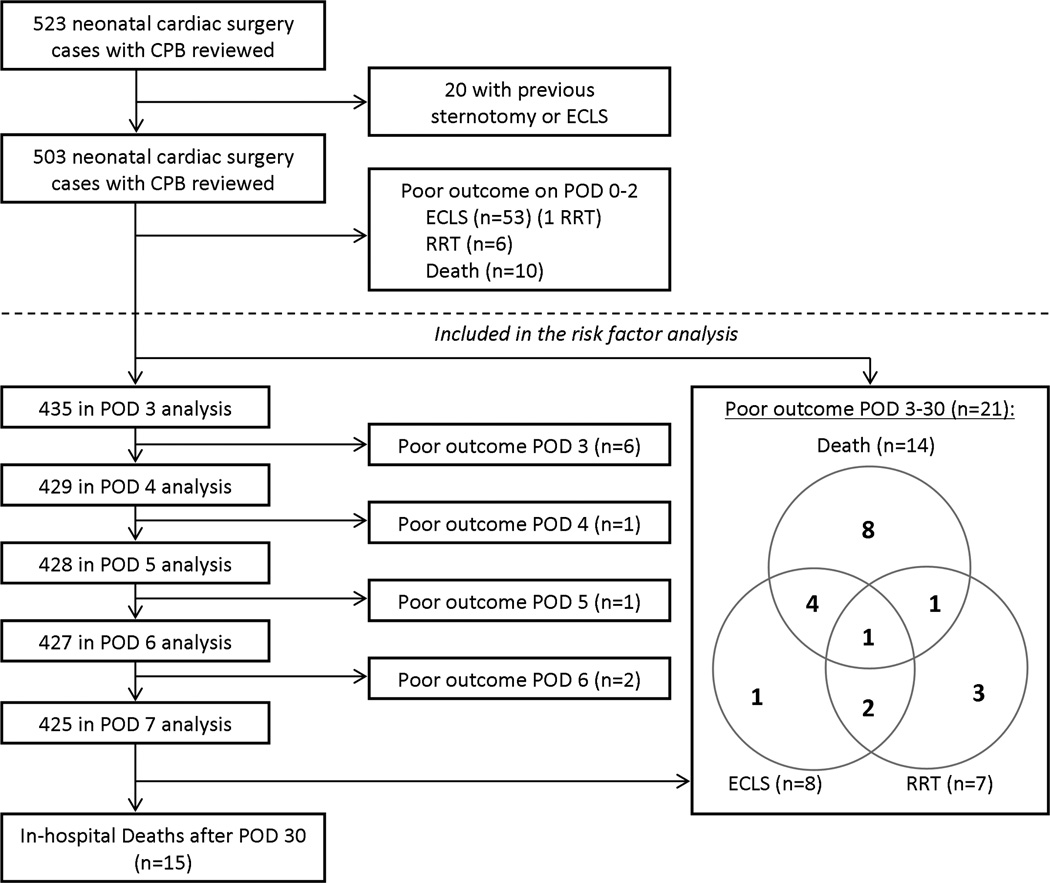
Patients: Four hundred thirty-five neonates undergoing cardiac surgery with cardiopulmonary bypass from January 2006 through December 2010.
Interventions: None.
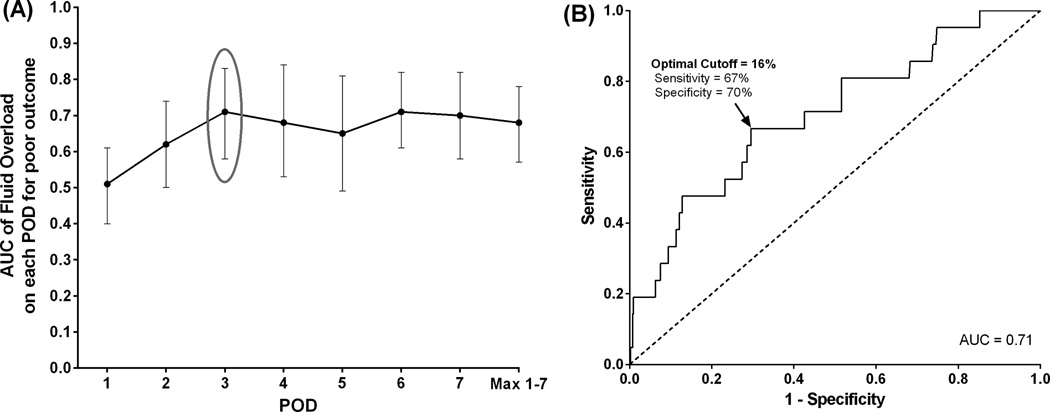
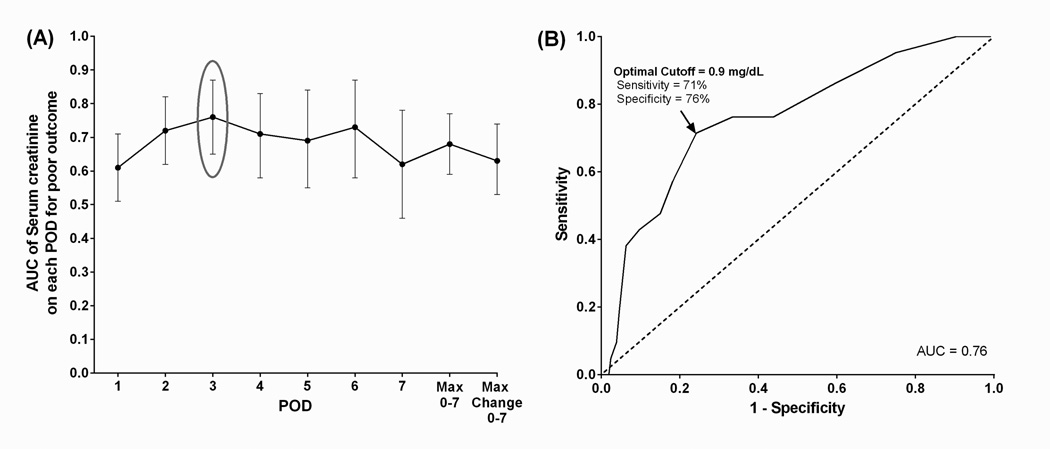
Measurements and main results: Demographics, diagnosis, and perioperative clinical variables were collected, including daily weights and serum creatinine levels. A composite poor clinical outcome (death, need for renal replacement therapy or extracorporeal life support within 30 postoperative days) was considered the primary outcome measure. Twenty-one neonates (5%) had a composite poor outcome with 7 (2%) requiring renal replacement therapy, 8 (2%) requiring extracorporeal life support, and 14 (3%) dying between 3 and 30 days post surgery. Neonates with a composite poor outcome had significantly higher maximum fluid overload (> 20%) and were slower to diurese. A receiver-operating characteristic curve determined that fluid overload greater than or equal to 16% and serum creatinine greater than or equal to 0.9 on postoperative day 3 were the optimal cutoffs for significant discrimination on the primary outcome (area under the curve = 0.71 and 0.76, respectively). In multivariable analysis, fluid overload greater than or equal to 16% (adjusted odds ratio = 3.7) and serum creatinine adjusted odds ratio 0.9 (adjusted odds ratio = 6.6) on postoperative day 3 remained an independent risk factor for poor outcome. Fluid overload greater than or equal 16% was also significantly associated with cardiac arrest requiring cardiopulmonary resuscitation, prolonged ICU stay, and chest reexploration.
Conclusions: This study highlights the importance of monitoring fluid balance in the neonatal cardiac surgical population and suggests that daily fluid overload, a readily available, noninvasive marker of renal function, may be a sensitive and specific predictor of adverse outcomes.
Figures
Comment in
-
Fluid Overload After Neonatal Cardiac Surgery Is Bad: Keep the Bottles on the Shelf, Squeeze the Patients…or Both?Pediatr Crit Care Med. 2016 May;17(5):463-5. doi: 10.1097/PCC.0000000000000720. Pediatr Crit Care Med. 2016. PMID: 27144694 No abstract available.
References
-
- Blinder JJ, Goldstein SL, Lee V-V, et al. Congenital heart surgery in infants: Effects of acute kidney injury on outcomes. J Thorac Cardiovasc Surg. 2012;143(2):368–374. - PubMed
-
- Chiravuri SD, Voepel-Lewis T, Devaney EJ, et al. The use of aprotinin in children undergoing operative repair of isolated atrial septal defects. Paediatr Anaesth. 2008;18(2):145–150. - PubMed
-
- Kist-van Holthe tot Echten JE, Goedvolk CA, Doornaar MB, et al. Acute renal insufficiency and renal replacement therapy after pediatric cardiopulmonary bypass surgery. Pediatr Cardiol. 2001;22(4):321–326. - PubMed
-
- Picca S, Principato F, Mazzera E, et al. Risks of acute renal failure after cardiopulmonary bypass surgery in children: a retrospective 10-year case-control study. Nephrol Dial Transplant. 1995;10(5):630–636. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
