

A multiplexed analysis approach identifies new association of inflammatory proteins in patients with overactive bladder
- PMID: 27029431
- PMCID: PMC4967156
- DOI: 10.1152/ajprenal.00580.2015
A multiplexed analysis approach identifies new association of inflammatory proteins in patients with overactive bladder
Abstract
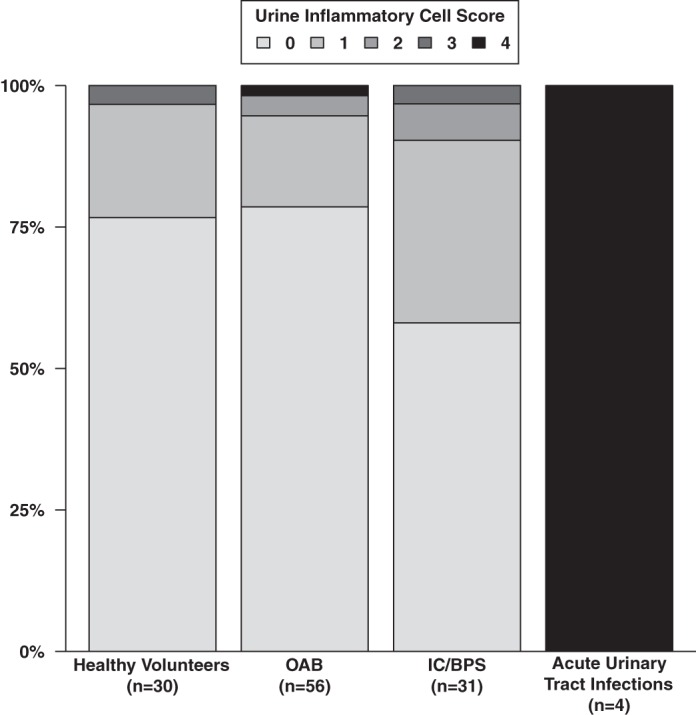
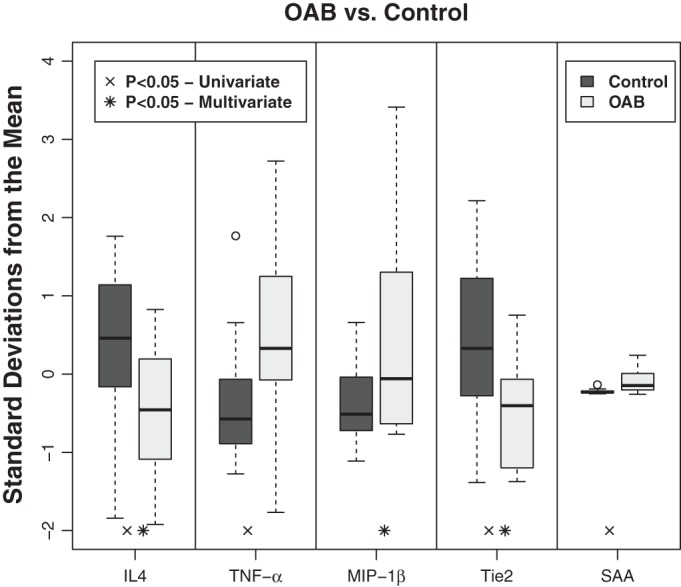
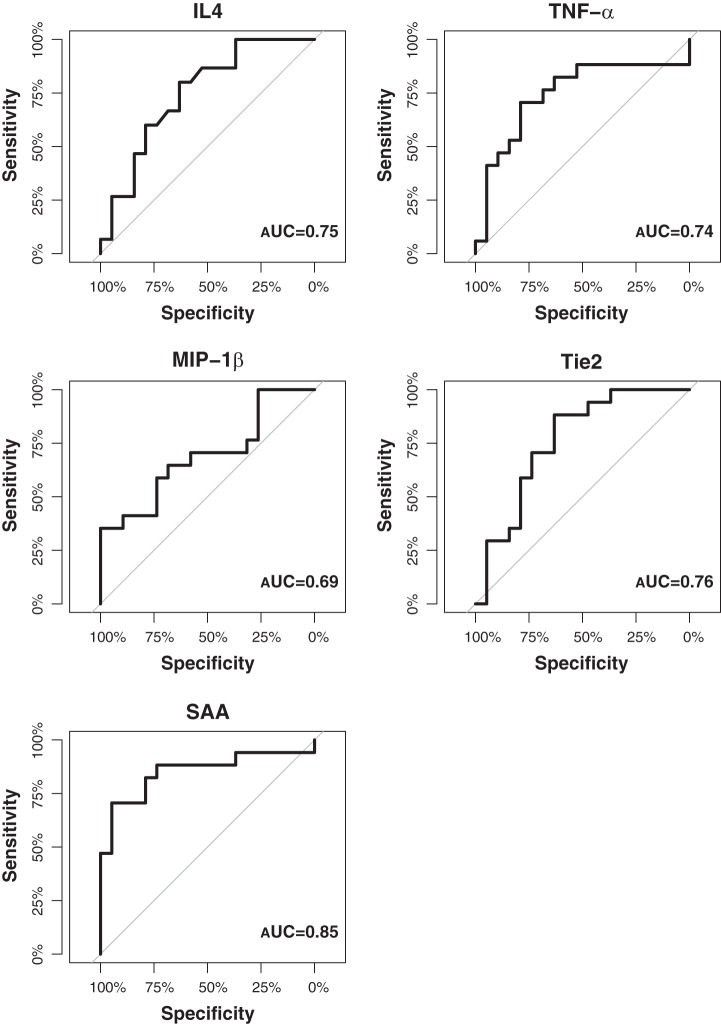
Overactive bladder (OAB) is a common debilitating bladder condition with unknown etiology and limited diagnostic modalities. Here, we explored a novel high-throughput and unbiased multiplex approach with cellular and molecular components in a well-characterized patient cohort to identify biomarkers that could be reliably used to distinguish OAB from controls or provide insights into underlying etiology. As a secondary analysis, we determined whether this method could discriminate between OAB and other chronic bladder conditions. We analyzed plasma samples from healthy volunteers (n = 19) and patients diagnosed with OAB, interstitial cystitis/bladder pain syndrome (IC/BPS), or urinary tract infections (UTI; n = 51) for proinflammatory, chemokine, cytokine, angiogenesis, and vascular injury factors using Meso Scale Discovery (MSD) analysis and urinary cytological analysis. Wilcoxon rank-sum tests were used to perform univariate and multivariate comparisons between patient groups (controls, OAB, IC/BPS, and UTI). Multivariate logistic regression models were fit for each MSD analyte on 1) OAB patients and controls, 2) OAB and IC/BPS patients, and 3) OAB and UTI patients. Age, race, and sex were included as independent variables in all multivariate analysis. Receiver operating characteristic (ROC) curves were generated to determine the diagnostic potential of a given analyte. Our findings demonstrate that five analytes, i.e., interleukin 4, TNF-α, macrophage inflammatory protein-1β, serum amyloid A, and Tie2 can reliably differentiate OAB relative to controls and can be used to distinguish OAB from the other conditions. Together, our pilot study suggests a molecular imbalance in inflammatory proteins may contribute to OAB pathogenesis.
Keywords: OAB; UTI; biomarkers; bladder pain syndrome; interstitial cystitis.
Copyright © 2016 the American Physiological Society.
Figures
References
-
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Am J Obstet Gynecol 187: 116–126, 2002. - PubMed
-
- Antunes-Lopes T, Pinto R, Barros SC, Botelho F, Silva CM, Cruz CD, Cruz F. Urinary neurotrophic factors in healthy individuals and patients with overactive bladder. J Urol 189: 359–365, 2013. - PubMed
-
- Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourol Urodyn 23: 322–330, 2004. - PubMed
-
- Bhide AA, Cartwright R, Khullar V, Digesu GA. Biomarkers in overactive bladder. Int Urogynecol J 24: 1065–1072, 2013. - PubMed
-
- Chen CL, Lin TS, Tsai CH, Wu CC, Chung T, Chien KY, Wu M, Chang YS, Yu JS, Chen YT. Identification of potential bladder cancer markers in urine by abundant-protein depletion coupled with quantitative proteomics. J Proteomics 85: 28–43, 2013. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous