

Magnetic resonance imaging findings of cellular angiofibroma of the tunica vaginalis of the testis: a case report
- PMID: 27029567
- PMCID: PMC4815127
- DOI: 10.1186/s13256-016-0861-3
Magnetic resonance imaging findings of cellular angiofibroma of the tunica vaginalis of the testis: a case report
Abstract
Background: Cellular angiofibroma represents a rare mesenchymal tumor typically involving the inguinoscrotal area in middle-aged men. Although the origin of this benign tumor is unknown, it is histologically classified as an angiomyxoid tumor. Cellular angiofibroma is characterized by a diversity of pathological and imaging features. An accurate preoperative diagnosis is challenging. Magnetic resonance imaging examination of the scrotum has been reported as a valuable adjunct modality in the investigation of scrotal pathology. The technique by providing both structural and functional information is useful in the differentiation between extratesticular and intratesticular diseases and in the preoperative characterization of the histologic nature of various scrotal lesions. There are few reports in the English literature addressing the magnetic resonance imaging findings of cellular angiofibroma of the scrotum and no reports on functional magnetic resonance imaging data. Here we present the first case of a cellular angiofibroma arising from the tunica vaginalis of the testis and we discuss the value of a multiparametric magnetic resonance protocol, including diffusion-weighted imaging, magnetization transfer imaging and dynamic contrast-enhanced magnetic resonance imaging in the preoperative diagnosis of this rare neoplasm.
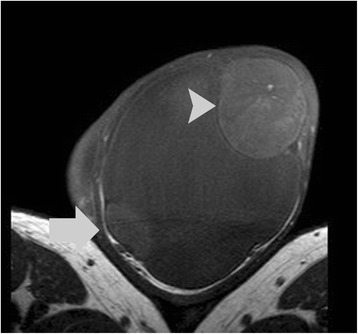
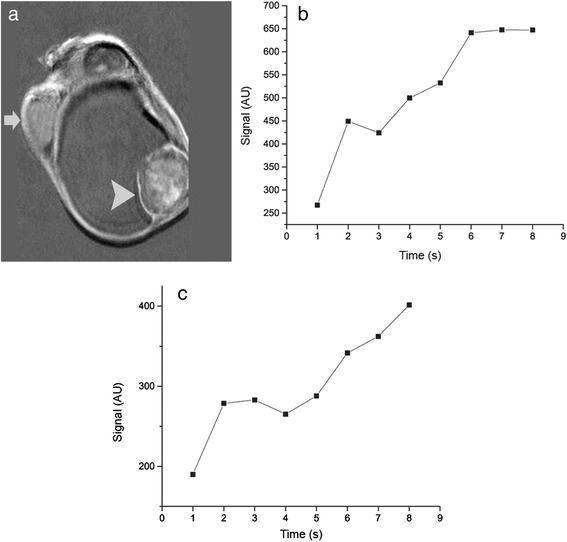
Case presentation: A 47-year Greek man presented with a painless left scrotal swelling, which had gradually enlarged during the last 6 months. Magnetic resonance imaging of his scrotum displayed a left paratesticular mass, in close proximity to the tunica vaginalis, with heterogeneous high signal intensity on T2-weighted images and no areas of restricted diffusion. The tumor was hypointense on magnetization transfer images, suggestive for the presence of macromolecules. On dynamic contrast-enhanced magnetic resonance imaging the mass showed intense heterogeneous enhancement with a type II curve. Magnetic resonance imaging findings were strongly suggestive of a benign paratesticular tumor, which was confirmed on pathology following lesion excision.
Conclusions: Magnetic resonance imaging of the scrotum by combining conventional and functional magnetic resonance data provides useful diagnostic information in the preoperative characterization of scrotal masses. A possible diagnosis of a benign paratesticular tumor based on magnetic resonance imaging features may improve patient care and decrease the number of unnecessary radical surgical explorations.
Keywords: Cellular angiofibroma; Diffusion-weighted MRI; Magnetic resonance; Magnetization transfer contrast imaging; Tunica vaginalis.
Figures




Similar articles
-
Conventional and diffusion-weighted magnetic resonance imaging findings of benign fibromatous paratesticular tumor: a case report.J Med Case Rep. 2011 May 3;5:169. doi: 10.1186/1752-1947-5-169. J Med Case Rep. 2011. PMID: 21539739 Free PMC article.
-
Para-testicular cellular angiofibroma: a rare tumour in a male renal transplant patient.Virchows Arch. 2006 Oct;449(4):489-92. doi: 10.1007/s00428-006-0289-z. Epub 2006 Sep 7. Virchows Arch. 2006. PMID: 16957933
-
Paratesticular cellular angiofibroma: a case report.J Med Case Rep. 2024 Apr 11;18(1):170. doi: 10.1186/s13256-024-04499-y. J Med Case Rep. 2024. PMID: 38600580 Free PMC article.
-
MRI of testicular malignancies.Abdom Radiol (NY). 2019 Mar;44(3):1070-1082. doi: 10.1007/s00261-018-1816-5. Abdom Radiol (NY). 2019. PMID: 30386879 Review.
-
[A cyst arising from tunica vaginalis testis : report of a case].Hinyokika Kiyo. 2011 Jun;57(6):341-4. Hinyokika Kiyo. 2011. PMID: 21795840 Review. Japanese.
Cited by
-
A case of inguinal cellular angiofibroma.IJU Case Rep. 2020 Feb 20;3(2):69-71. doi: 10.1002/iju5.12147. eCollection 2020 Mar. IJU Case Rep. 2020. PMID: 32743474 Free PMC article.
-
Spindle Cell Lipoma and Pleomorphic Lipoma: An Update and Review.Cancer Diagn Progn. 2023 May 3;3(3):282-290. doi: 10.21873/cdp.10213. eCollection 2023 May-Jun. Cancer Diagn Progn. 2023. PMID: 37168965 Free PMC article. Review.
-
Imaging of the scrotum: beyond sonography.Insights Imaging. 2018 Apr;9(2):137-148. doi: 10.1007/s13244-017-0592-z. Epub 2018 Feb 15. Insights Imaging. 2018. PMID: 29450854 Free PMC article. Review.
-
Cellular Angiofibroma of the Perineal Region With Tortuous Vessels: A Report of Three Cases.Cureus. 2025 Mar 21;17(3):e80969. doi: 10.7759/cureus.80969. eCollection 2025 Mar. Cureus. 2025. PMID: 40255726 Free PMC article.
-
Combined classical spindle cell/pleomorphic lipoma spectrum imaging and clinical data.Skeletal Radiol. 2018 Jan;47(1):51-59. doi: 10.1007/s00256-017-2751-1. Epub 2017 Aug 19. Skeletal Radiol. 2018. PMID: 28823067
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
