

Graves' disease in a mediastinal mass presenting after total thyroidectomy for nontoxic multinodular goiter: a case report
- PMID: 27029843
- PMCID: PMC4815244
- DOI: 10.1186/s13256-016-0878-7
Graves' disease in a mediastinal mass presenting after total thyroidectomy for nontoxic multinodular goiter: a case report
Abstract
Background: Thyrotoxicosis after total thyroidectomy is mostly iatrogenic. Rarely, a hyperfunctional thyroid remnant or ectopic tissue may be the cause. There are few cases of Graves' disease arising from thyroid tissue located in the mediastinum and none in which Graves' disease was diagnosed only after surgery. We report the case of a patient with Graves's disease in a mediastinal thyroid mass presenting 7 years after total thyroidectomy for nontoxic goiter.
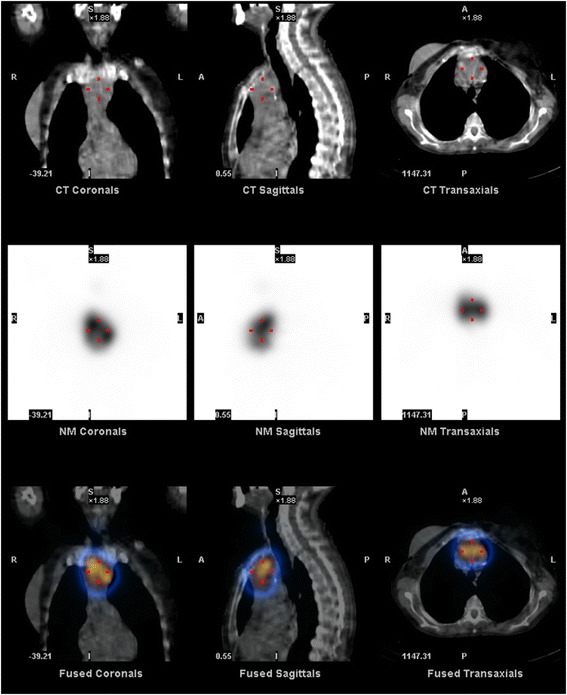
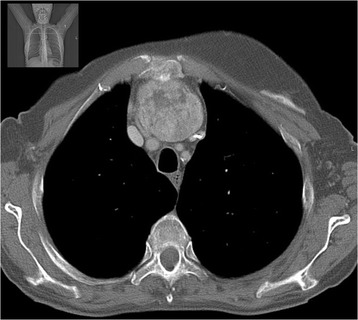
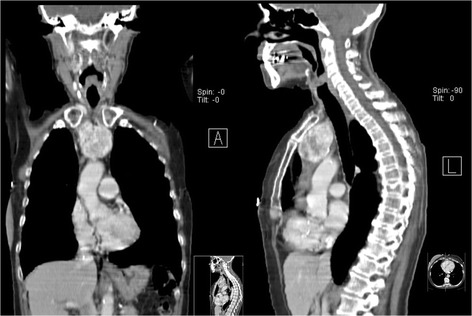
Case presentation: A 67-year-old Caucasian woman presented with palpitations, fatigue and weight loss. She had a history of total thyroidectomy for nontoxic multinodular goiter at the age of 60 without any signs of malignancy on microscopic examination. She had been medicated with levothyroxine 100 μg/day since the surgery without follow-up. She was tachycardic, had no cervical mass or eye involvement. Her thyroid-stimulating hormone levels were suppressed (0.000 μU/mL) and her free thyroxine (3.22 ng/dL) and free triiodothyronine (8.46 pg/mL) levels increased. Neither mediastinal enlargement nor trachea deviation was found on chest roentgenogram. Levothyroxine treatment was stopped but our patient showed no improvement on free thyroxine or free triiodothyronine 10 days later. Thyroglobulin was increased to 294 mg/mL. A cervical ultrasound scan revealed no thyroid remnant. Her anti-thyroid-stimulating hormone receptor antibodies were high (19.7 U/L). Corporal scintigraphy demonstrated increased intrathoracic radioiodine uptake. A computed tomography scan confirmed a 60 × 40 mm mediastinal mass. Methimazole 10 mg/day was started. Three months later, her thyroid function was normal and she underwent surgical resection. Microscopic examination showed thyroid tissue with no signs of malignancy.
Conclusions: Although thyrotoxicosis after total thyroidectomy is mostly due to excessive supplementation, true hyperthyroidism may rarely be the cause, which should be kept in mind. The presence of thyroid tissue after total thyroidectomy in our patient may correspond to a remnant or ectopic thyroid tissue that became hyperfunctional in the presence of anti- thyroid-stimulating hormone receptor antibodies.
Keywords: Graves’ disease; Hyperthyroidism; Mediastinal mass; Thyroid remnant; Total thyroidectomy.
Figures
References
-
- Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. 2011;17:456–520. doi: 10.4158/EP.17.3.456. - DOI - PubMed
-
- Calo PG, Tatti A, Medas F, Petruzzo P, Pisano G, Nicolosi A. Forgotten goiter. Our experience and a review of the literature. Ann Ital Chir. 2012;83:487–90. - PubMed
-
- D’Andrea V, Cantisani V, Catania A, Di Matteo FM, Sorrenti S, Greco R, et al. Thyroid tissue remnants after “total thyroidectomy”. G Chir. 2009;30:339–44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
