

Diagnostic Accuracy of the Small Membrane Filtration Method for Diagnosis of Pulmonary Tuberculosis in a High-HIV-Prevalence Setting
- PMID: 27030493
- PMCID: PMC4879284
- DOI: 10.1128/JCM.00017-16
Diagnostic Accuracy of the Small Membrane Filtration Method for Diagnosis of Pulmonary Tuberculosis in a High-HIV-Prevalence Setting
Abstract
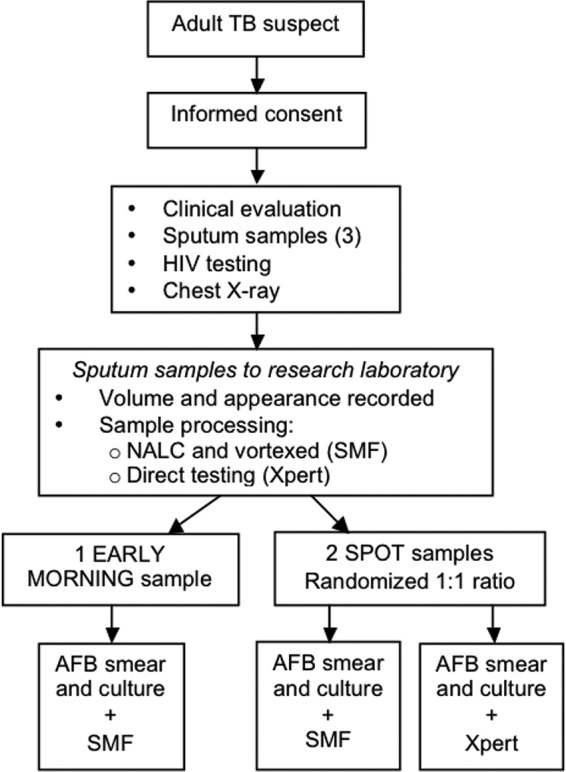
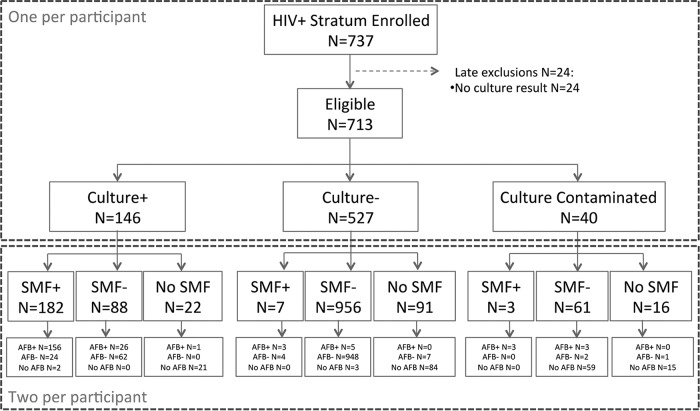
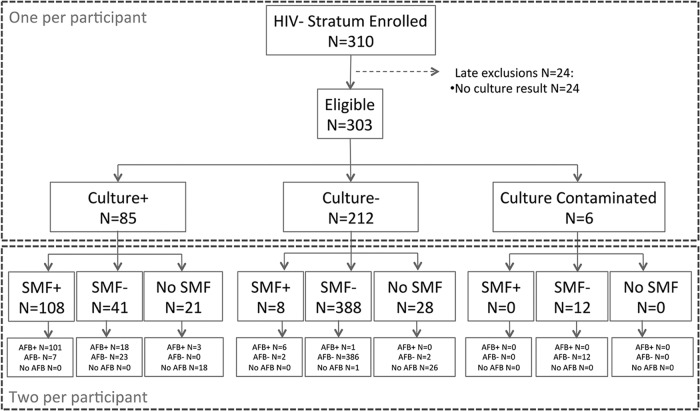
Sputum acid-fast bacilli (AFB) smear microscopy has suboptimal sensitivity but remains the most commonly used laboratory test to diagnose pulmonary tuberculosis (TB). We prospectively evaluated the small membrane filtration (SMF) method that concentrates AFB in a smaller area to facilitate detection to improve the diagnostic performance of microscopy. We enrolled adults with suspicion of pulmonary TB from health facilities in southwestern Uganda. Clinical history, physical examination, and 3 sputum samples were obtained for direct fluorescent AFB smear, SMF, Xpert MTB/RIF, and MGIT culture media. Sensitivity and specificity were estimated for SMF, AFB smear, and Xpert MTB/RIF, using MGIT as the reference standard. The analysis was stratified according to HIV status. From September 2012 to April 2014, 737 participants were included in the HIV-infected stratum (146 [20.5%] were culture positive) and 313 were in the HIV-uninfected stratum (85 [28%] were culture positive). In HIV-infected patients, the sensitivity of a single SMF was 67.4% (95% confidence interval [CI], 59.9% to 74.1%); for AFB, 68.0% (95% CI, 60.6% to 74.6%); and for Xpert MTB/RIF, 91.0% (95% CI, 85.0% to 94.8%). In HIV-uninfected patients, the corresponding sensitivities were 72.5% (95% CI, 62.1% to 80.9%), 80.3% (95% CI, 70.8% to 87.2%), and 93.5% (95% CI, 85.7% to 97.2%). The specificity for all 3 tests in both HIV groups was ≥96%. In this setting, the SMF method did not improve the diagnostic accuracy of sputum AFB. The Xpert MTB/RIF assay performed well in both HIV-infected and -uninfected groups.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Trébucq A. 2004. Revisiting sputum smear microscopy. Int J Tuberc Lung Dis 8:805. - PubMed
-
- Shaw JB, Wynn-Williams N. 1954. Infectivity of pulmonary tuberculosis in relation to sputum status. Am Rev Tuberc 69:724–732. - PubMed
-
- Davies PD, Pai M. 2008. The diagnosis and misdiagnosis of tuberculosis. Int J Tuberc Lung Dis 12:1226–1234. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
