

Spinal nociceptive transmission by mechanical stimulation of bone marrow
- PMID: 27030710
- PMCID: PMC4994861
- DOI: 10.1177/1744806916628773
Spinal nociceptive transmission by mechanical stimulation of bone marrow
Abstract
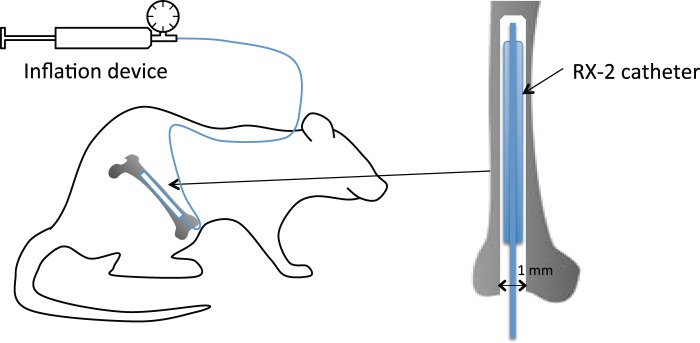
Background: Since bone marrow receives innervation from A-delta and C-fibers and since an increase in intramedullary pressure in bone marrow may induce acute pain in orthopedic patients during surgery and chronic pain in patients with bone marrow edema, skeletal pain may partly originate from bone marrow. Intraosseous lesions, such as osteomyelitis and bone cancer, are also known to produce cutaneous hypersensitivity, which might be referred pain from bone. However, little is known about pain perception in bone marrow and referred pain induced by bone disease. Thus, we carried out an in vivo electrophysiological study and behavioral study to determine whether increased intraosseous pressure of the femur induces acute pain and whether increased intraosseous pressure induces referred pain in the corresponding receptive fields of the skin.
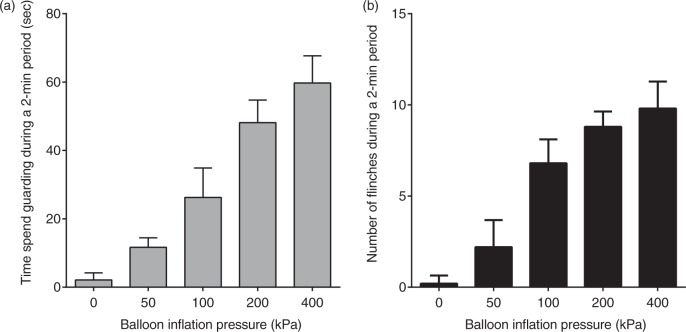
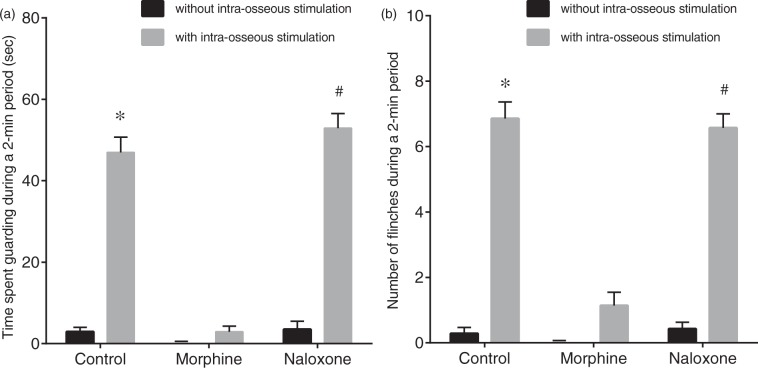
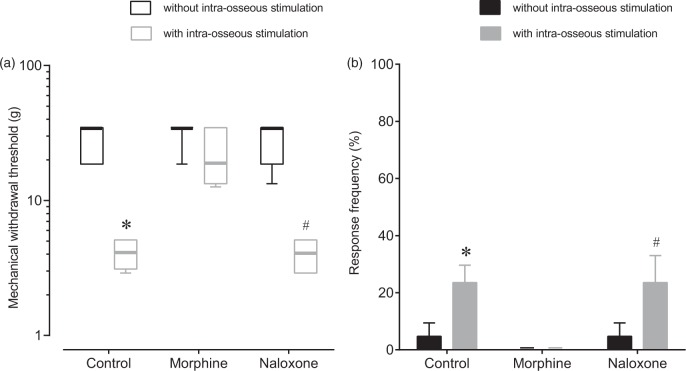
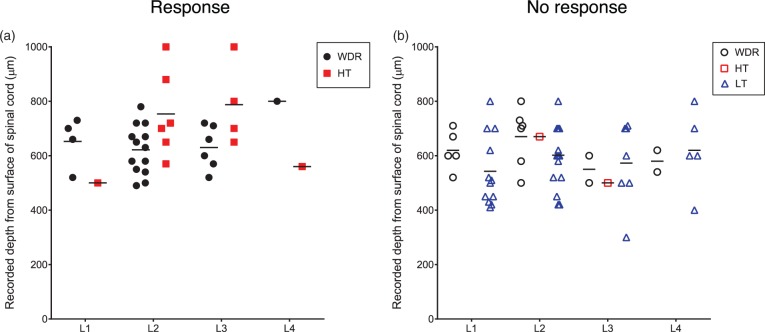
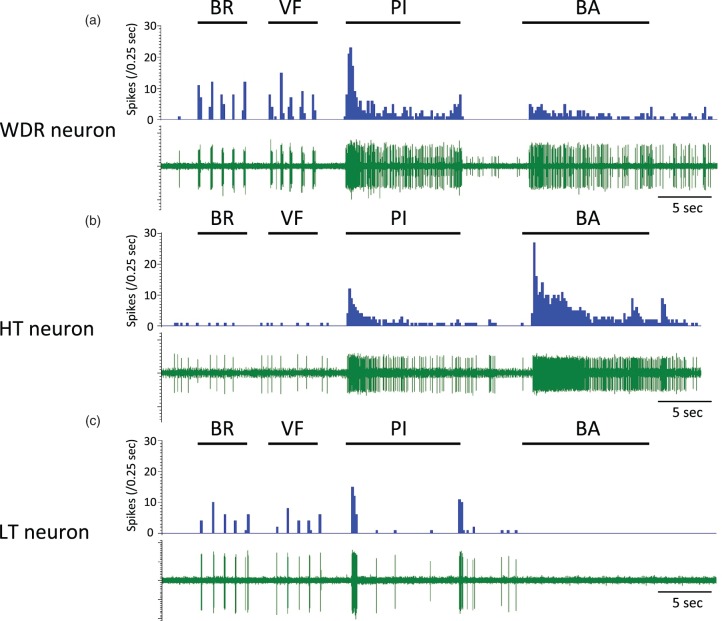
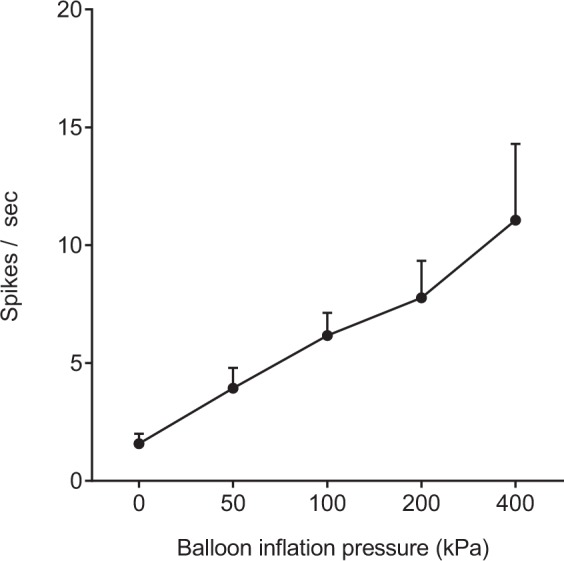
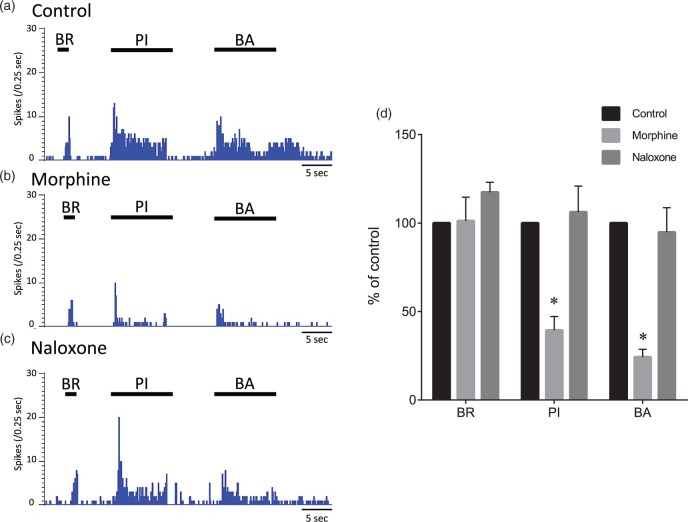
Results: Intraosseous balloon inflation caused spontaneous pain-related behavior and mechanical hyperalgesia and allodynia in the lumbosacral region. Single neuronal activities of spinal dorsal horn neurons were extracellularly isolated, and then evoked responses to non-noxious and noxious cutaneous stimuli and intraosseous balloon inflation were recorded. Ninety-four spinal dorsal horn neurons, which had somatic receptive fields at the lower back and thigh, were obtained. Sixty-two percent of the wide-dynamic-range neurons (24/39) and 86% of the high-threshold neurons (12/14) responded to intraosseous balloon inflation, while none of the low-threshold neurons (0/41) responded to intraosseous balloon inflation. Spinally administered morphine (1 µg) abolished balloon inflation-induced spontaneous pain-related behavior and mechanical hyperalgesia in awake rats and also suppressed evoked activities of wide-dynamic-range neurons to noxious cutaneous stimulation and intraosseous balloon inflation.
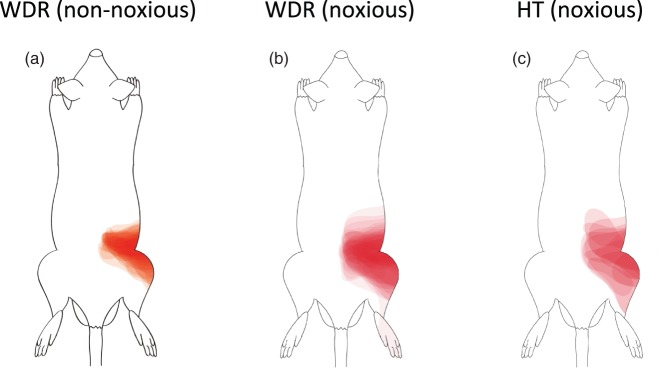
Conclusions: The results suggest that mechanical stimulation to bone marrow produces nociception, concomitantly producing its referred pain in the corresponding skin fields. These mechanisms might contribute to pain caused by skeletal diseases.
Keywords: Skeletal pain; in vivo electrophysiology; referred pain.
© The Author(s) 2016.
Figures
Similar articles
-
Changes in properties of spinal dorsal horn neurons and their sensitivity to morphine after spinal cord injury in the rat.Anesthesiology. 2005 Jan;102(1):152-64. doi: 10.1097/00000542-200501000-00024. Anesthesiology. 2005. PMID: 15618799
-
Cellular mechanisms of hyperalgesia and spontaneous pain in a spinalized rat model of peripheral neuropathy: changes in myelinated afferent inputs implicated.Eur J Neurosci. 2000 Jun;12(6):2006-20. doi: 10.1046/j.1460-9568.2000.00087.x. Eur J Neurosci. 2000. PMID: 10886340
-
A neuronal correlate of secondary hyperalgesia in the rat spinal dorsal horn is submodality selective and facilitated by supraspinal influence.Exp Neurol. 1998 Jan;149(1):193-202. doi: 10.1006/exnr.1997.6688. Exp Neurol. 1998. PMID: 9454628
-
Chronic spinal nerve ligation induces changes in response characteristics of nociceptive spinal dorsal horn neurons and in their descending regulation originating in the periaqueductal gray in the rat.Exp Neurol. 1997 Oct;147(2):428-36. doi: 10.1006/exnr.1997.6555. Exp Neurol. 1997. PMID: 9344567
-
Exogenous tumor necrosis factor-alpha induces abnormal discharges in rat dorsal horn neurons.Spine (Phila Pa 1976). 2002 Aug 1;27(15):1618-24; discussion 1624. doi: 10.1097/00007632-200208010-00005. Spine (Phila Pa 1976). 2002. PMID: 12163721
Cited by
-
Sensitization of Cutaneous Primary Afferents in Bone Cancer Revealed by In Vivo Calcium Imaging.Cancers (Basel). 2020 Nov 24;12(12):3491. doi: 10.3390/cancers12123491. Cancers (Basel). 2020. PMID: 33255209 Free PMC article.
-
Skin cooling and topical application of menthol can reduce propofol injection-induced pain, a randomized trial.Medicine (Baltimore). 2025 Jun 13;104(24):e42809. doi: 10.1097/MD.0000000000042809. Medicine (Baltimore). 2025. PMID: 40527818 Free PMC article. Clinical Trial.
-
Stomatin-like protein 3 modulates the responses of Aδ, but not C fiber bone afferent neurons to noxious mechanical stimulation in an animal model of acute experimental bone pain.Mol Pain. 2023 Jan-Dec;19:17448069231222407. doi: 10.1177/17448069231222407. Mol Pain. 2023. PMID: 38073226 Free PMC article.
-
The Functional and Morphological Changes of the Cervical Intervertebral Disc after Applying Lordotic Curve Controlled Traction: A Double-Blind Randomized Controlled Study.Int J Environ Res Public Health. 2019 Jun 19;16(12):2162. doi: 10.3390/ijerph16122162. Int J Environ Res Public Health. 2019. PMID: 31248064 Free PMC article. Clinical Trial.
-
Piezo2 Knockdown Inhibits Noxious Mechanical Stimulation and NGF-Induced Sensitization in A-Delta Bone Afferent Neurons.Front Physiol. 2021 Jul 15;12:644929. doi: 10.3389/fphys.2021.644929. eCollection 2021. Front Physiol. 2021. PMID: 34335288 Free PMC article.
References
-
- Forley KM. Pain assessment and cancer pain syndromes. In: Doyle D, Hanks GW, MacDonald N. (eds). Oxford textbook of palliative medicine, 2nd ed Oxford: Oxford Medical Publications, 1998, pp. 310–331.
-
- Bazett HC, McGlone B. Note on the pain sensations which accompany deep punctures. Brain 1928; 51: 18–23.
-
- Tabarowski Z, Gibson-Berry K, Felten SY. Noradrenergic and peptidergic innervation of the mouse femur bone marrow. Acta Histochem 1996; 98: 453–457. - PubMed
-
- Mach DB, Rogers SD, Sabino MC, et al. Origins of skeletal pain: sensory and sympathetic innervation of the mouse femur. Neuroscience 2002; 113: 155–166. - PubMed
-
- Ivanusic JJ. The pattern of Fos expression in the spinal dorsal horn following acute noxious mechanical stimulation of bone. Eur J Pain 2008; 12: 895–899. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
