

Athletic Cardiac Adaptation in Males Is a Consequence of Elevated Myocyte Mass
- PMID: 27033835
- PMCID: PMC4841180
- DOI: 10.1161/CIRCIMAGING.115.003579
Athletic Cardiac Adaptation in Males Is a Consequence of Elevated Myocyte Mass
Abstract
Background: Cardiac remodeling occurs in response to regular athletic training, and the degree of remodeling is associated with fitness. Understanding the myocardial structural changes in athlete's heart is important to develop tools that differentiate athletic from cardiomyopathic change. We hypothesized that athletic left ventricular hypertrophy is a consequence of increased myocardial cellular rather than extracellular mass as measured by cardiovascular magnetic resonance.
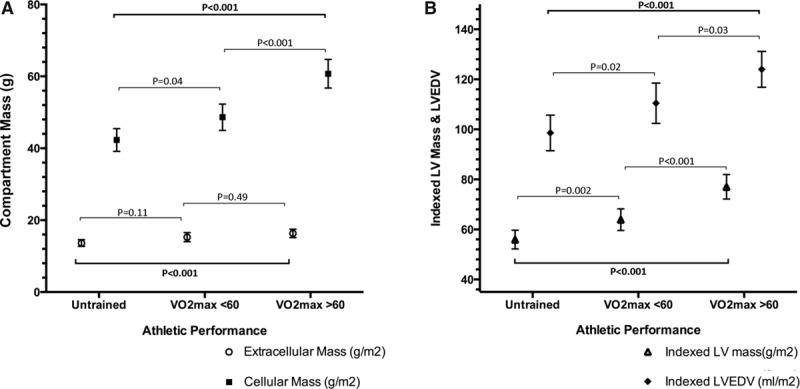
Methods and results: Forty-five males (30 athletes and 15 sedentary age-matched healthy controls) underwent comprehensive cardiovascular magnetic resonance studies, including native and postcontrast T1 mapping for extracellular volume calculation. In addition, the 30 athletes performed a maximal exercise test to assess aerobic capacity and anaerobic threshold. Participants were grouped by athleticism: untrained, low performance, and high performance (O2max <60 or>60 mL/kg per min, respectively). In athletes, indexed cellular mass was greater in high- than low-performance athletes 60.7±7.5 versus 48.6±6.3 g/m(2); P<0.001), whereas extracellular mass was constant (16.3±2.2 versus 15.3±2.2 g/m(2); P=0.20). Indexed left ventricular end-diastolic volume and mass correlated with O2max (r=0.45, P=0.01; r=0.55, P=0.002) and differed significantly by group (P=0.01; P<0.001, respectively). Extracellular volume had an inverse correlation with O2max (r=-0.53, P=0.003 and left ventricular mass index (r=-0.44, P=0.02).
Conclusions: Increasing left ventricular mass in athlete's heart occurs because of an expansion of the cellular compartment while the extracellular volume becomes relatively smaller: a difference which becomes more marked as left ventricular mass increases. Athletic remodeling, both on a macroscopic and cellular level, is associated with the degree of an individual's fitness. Cardiovascular magnetic resonance ECV quantification may have a future role in differentiating athlete's heart from change secondary to cardiomyopathy.
Keywords: ECV; T1 mapping; athlete’s heart; cardiovascular magnetic resonance imaging; exercise physiology; hypertrophy/remodeling.
© 2016 The Authors.
Figures
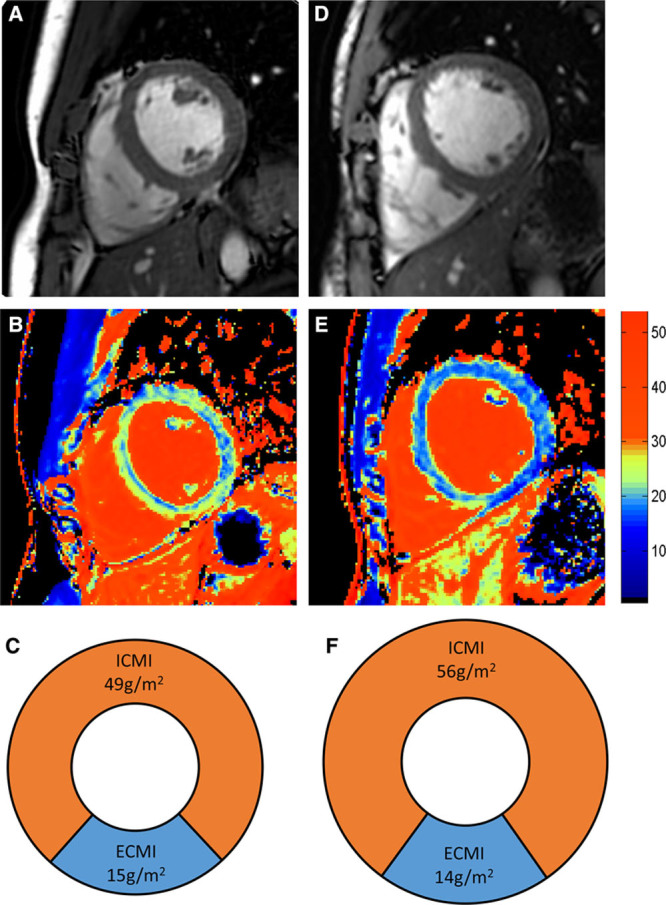
 O2max of 50 mL/kg per in, and right column shows a high-performance athlete with a
O2max of 50 mL/kg per in, and right column shows a high-performance athlete with a  O2max of 75 mL/kg per min. A and D, Short-axis images of left and right ventricle. B and E, extracellular volume (ECV) color maps showing lower ECV in the high performance athletes throughout the myocardium. C and F, Pie charts scaled to overall indexed LV mass displaying the relative indexed masses of the cellular and extracellular compartments (not short axis images). ECMI indicates indexed extracellular mass; and ICMI, indexed intracellular mass.
O2max of 75 mL/kg per min. A and D, Short-axis images of left and right ventricle. B and E, extracellular volume (ECV) color maps showing lower ECV in the high performance athletes throughout the myocardium. C and F, Pie charts scaled to overall indexed LV mass displaying the relative indexed masses of the cellular and extracellular compartments (not short axis images). ECMI indicates indexed extracellular mass; and ICMI, indexed intracellular mass.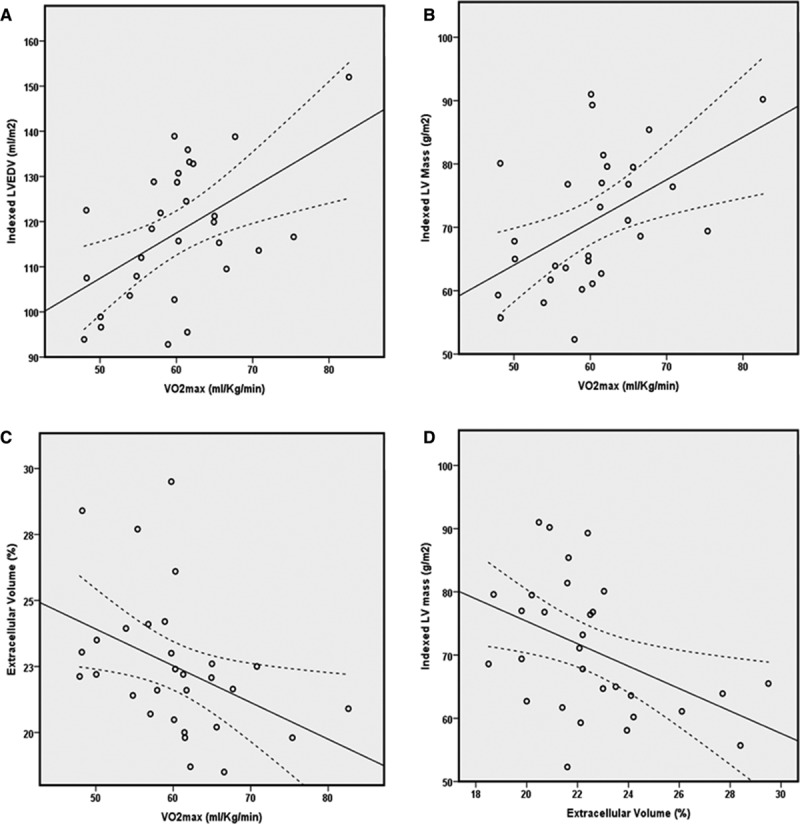
Comment in
-
T1 Mapping in Athletes: A Novel Tool to Differentiate Physiological Adaptation From Pathology?Circ Cardiovasc Imaging. 2016 Apr;9(4):e004706. doi: 10.1161/CIRCIMAGING.116.004706. Circ Cardiovasc Imaging. 2016. PMID: 27033836 No abstract available.
Similar articles
-
Morphological changes and myocardial function assessed by traditional and novel echocardiographic methods in preadolescent athlete's heart.Eur J Prev Cardiol. 2018 Jun;25(9):1000-1007. doi: 10.1177/2047487318776079. Epub 2018 May 22. Eur J Prev Cardiol. 2018. PMID: 29785884
-
Assessment of myocardial changes in athletes with native T1 mapping and cardiac functional evaluation using 3 T MRI.Int J Cardiovasc Imaging. 2016 Jun;32(6):975-81. doi: 10.1007/s10554-016-0866-4. Epub 2016 Feb 27. Int J Cardiovasc Imaging. 2016. PMID: 26920720
-
T1 and T2 mapping for early diagnosis of dilated non-ischaemic cardiomyopathy in middle-aged patients and differentiation from normal physiological adaptation.Eur Heart J Cardiovasc Imaging. 2016 Jul;17(7):797-803. doi: 10.1093/ehjci/jev216. Epub 2015 Sep 10. Eur Heart J Cardiovasc Imaging. 2016. PMID: 26358692
-
Left Ventricular Hypertrophy in Athletes: Differentiating Physiology From Pathology.Curr Treat Options Cardiovasc Med. 2018 Oct 26;20(12):96. doi: 10.1007/s11936-018-0691-2. Curr Treat Options Cardiovasc Med. 2018. PMID: 30367318 Review.
-
Diastolic function in various forms of left ventricular hypertrophy: contribution of active Doppler stress echo.Int J Sports Med. 1996 Nov;17 Suppl 3:S184-90. doi: 10.1055/s-2007-972922. Int J Sports Med. 1996. PMID: 9119541 Review.
Cited by
-
Myocardial tissue characterization and strain analysis in healthy pregnant women using cardiovascular magnetic resonance native T1 mapping and feature tracking technique.J Cardiovasc Magn Reson. 2018 Aug 2;20(1):52. doi: 10.1186/s12968-018-0476-5. J Cardiovasc Magn Reson. 2018. PMID: 30068369 Free PMC article.
-
Impact of Diabetes Mellitus on Ventricular Structure, Arterial Stiffness, and Pulsatile Hemodynamics in Heart Failure With Preserved Ejection Fraction.J Am Heart Assoc. 2019 Feb 19;8(4):e011457. doi: 10.1161/JAHA.118.011457. J Am Heart Assoc. 2019. PMID: 30764699 Free PMC article. Clinical Trial.
-
Multi-parametric assessment of left ventricular hypertrophy using late gadolinium enhancement, T1 mapping and strain-encoded cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2021 Jul 12;23(1):92. doi: 10.1186/s12968-021-00775-8. J Cardiovasc Magn Reson. 2021. PMID: 34247623 Free PMC article.
-
Native T1 mapping times are strongly influenced by elite athlete status.Eur Heart J Cardiovasc Imaging. 2025 Jun 30;26(7):1208-1216. doi: 10.1093/ehjci/jeaf123. Eur Heart J Cardiovasc Imaging. 2025. PMID: 40250969 Free PMC article.
-
CMR Mapping: The 4th-Era Revolution in Cardiac Imaging.J Clin Med. 2024 Jan 7;13(2):337. doi: 10.3390/jcm13020337. J Clin Med. 2024. PMID: 38256470 Free PMC article. Review.
References
-
- Harmon KG, Drezner JA, Wilson MG, Sharma S. Incidence of sudden cardiac death in athletes: a state-of-the-art review. Br J Sports Med. 2014;48:1185–1192. doi: 10.1136/bjsports-2014-093872. - PubMed
-
- Bellenger NG, Davies LC, Francis JM, Coats AJ, Pennell DJ. Reduction in sample size for studies of remodeling in heart failure by the use of cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2000;2:271–278. - PubMed
-
- Myerson SG, Bellenger NG, Pennell DJ. Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension. 2002;39:750–755. - PubMed
-
- Sado DM, Flett AS, Banypersad SM, White SK, Maestrini V, Quarta G, Lachmann RH, Murphy E, Mehta A, Hughes DA, McKenna WJ, Taylor AM, Hausenloy DJ, Hawkins PN, Elliott PM, Moon JC. Cardiovascular magnetic resonance measurement of myocardial extracellular volume in health and disease. Heart. 2012;98:1436–1441. doi: 10.1136/heartjnl-2012-302346. - PubMed
-
- Sado DM, White SK, Piechnik SK, Banypersad SM, Treibel T, Captur G, Fontana M, Maestrini V, Flett AS, Robson MD, Lachmann RH, Murphy E, Mehta A, Hughes D, Neubauer S, Elliott PM, Moon JC. Identification and assessment of Anderson-Fabry disease by cardiovascular magnetic resonance noncontrast myocardial T1 mapping. Circ Cardiovasc Imaging. 2013;6:392–398. doi: 10.1161/CIRCIMAGING.112.000070. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
