

Neoadjuvant chemoradiation followed by orthotopic liver transplantation in cholangiocarcinomas: the emory experience
- PMID: 27034793
- PMCID: PMC4783737
- DOI: 10.3978/j.issn.2078-6891.2015.117
Neoadjuvant chemoradiation followed by orthotopic liver transplantation in cholangiocarcinomas: the emory experience
Abstract
Background: Cholangiocarcinoma (CCA) is a bile duct tumor with a grim prognosis. The median survival after radiotherapy of unresectable disease is 9-12 months. The following is a review of our experience with neoadjuvant (NEO) chemoradiation followed by orthotopic liver transplantation (OLT) for CCA.
Methods: Ten patients with CCAs were selected as candidates for NEO-OLT between 2008-2011. Patients with unresectable CCA above the cystic duct without intra or extrahepatic metastases were eligible. Primary sclerosing cholangitis (PSC) patients were included due to their poor resection response. Patients initially received external-beam radiation [via conventional fields or volumetric-modulated arc therapy (VMAT)] plus capecitabine (XEL) or 5-fluorouracil (5-FU), followed by either Iridium(192) (Ir(192)) brachytherapy high dose rate (HDR) or external boost. 5-FU or XEL was administered until OLT. Patients underwent periodic surveillance computed tomography (CT)/MRIs after OLT. Primary endpoints included actuarial rates (AR)/crude rates (CR) of overall survival (OS), and local control (LC) at 6, 12, and 24 months.
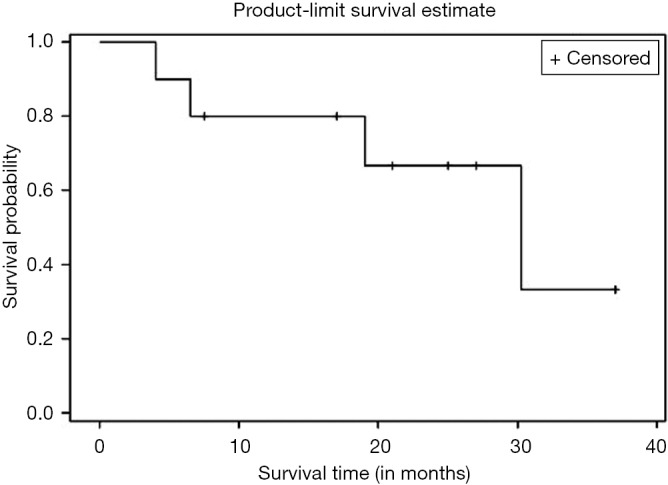
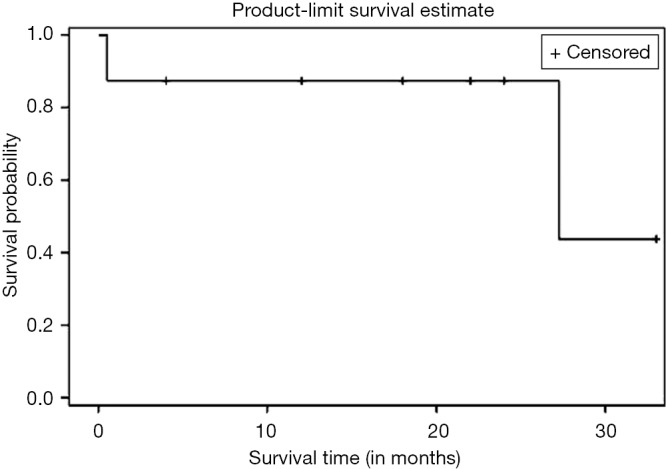
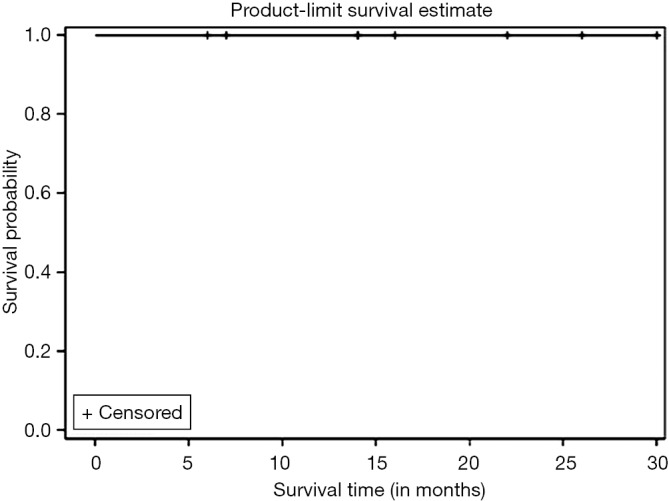
Results: Five males and five females were identified. Mean age was 58.3 years (range, 38-71 years). Mean composite radiation dose delivered was 59.0 Gy (range, 54-71.4 Gy). Forty percent of patients had an HDR boost. Fifty percent of patients received XEL during NEO. Two patients were excluded from the analysis as they did not go on to OLT due to metastases (n=1) and death due to GI bleed (n=1). Thirty-eight percent of the OLT patients had a pathological complete response (pCR) after NEO, while 25% required a Whipple due to positive margins. Median follow-up for the OLT group was 23 months (range, 6.5-37 months). Six, twelve, and twenty-four months LC AR was 100%. LC CR was 100% at longest interval (30 months). Six, twelve, and twenty-four months OS AR was 100%, 87.5%, and 87.5%, respectively. Mean OS AR was 30.2 months (95% CI: 22.8-37.7). OS CR was 75% at longest interval (37 months). Post OLT mortality resulted from (I) unknown causes (0.5 months), (II) allograft rejection (27.25 months). Other toxicities included: necrotic myelitis 12/10 months after NEO/OLT (n=1), post NEO biliary stricture requiring new stent (n=1); post Whipple bile leak repair (n=1), and post OLT fistula (n=1), cholangitis (n=1), and wound revision (n=2).
Conclusions: Our outcomes using NEO-OLT for CCA are promising and comparable to other series. These results further justify (I) use of NEO and (II) prioritization of available transplant livers for CCA management.
Keywords: Cholangiocarcinoma (CCA); chemoradiation; neoadjuvant (NEO); transplantation.
Conflict of interest statement
Figures
References
-
- Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. an unusual tumor with distinctive clinical and pathological features. Am J Med 1965;38:241-56. - PubMed
-
- Parker SL, Tong T, Bolden S, et al. Cancer statistics, 1996. CA Cancer J Clin 1996;46:5-27. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis 2004;24:115-25. - PubMed
-
- Hirohashi K, Uenishi T, Kubo S, et al. Macroscopic types of intrahepatic cholangiocarcinoma: clinicopathologic features and surgical outcomes. Hepatogastroenterology 2002;49:326-9. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials