

Surgical Approaches to First Branchial Cleft Anomaly Excision: A Case Series
- PMID: 27034873
- PMCID: PMC4789415
- DOI: 10.1155/2016/3902974
Surgical Approaches to First Branchial Cleft Anomaly Excision: A Case Series
Abstract
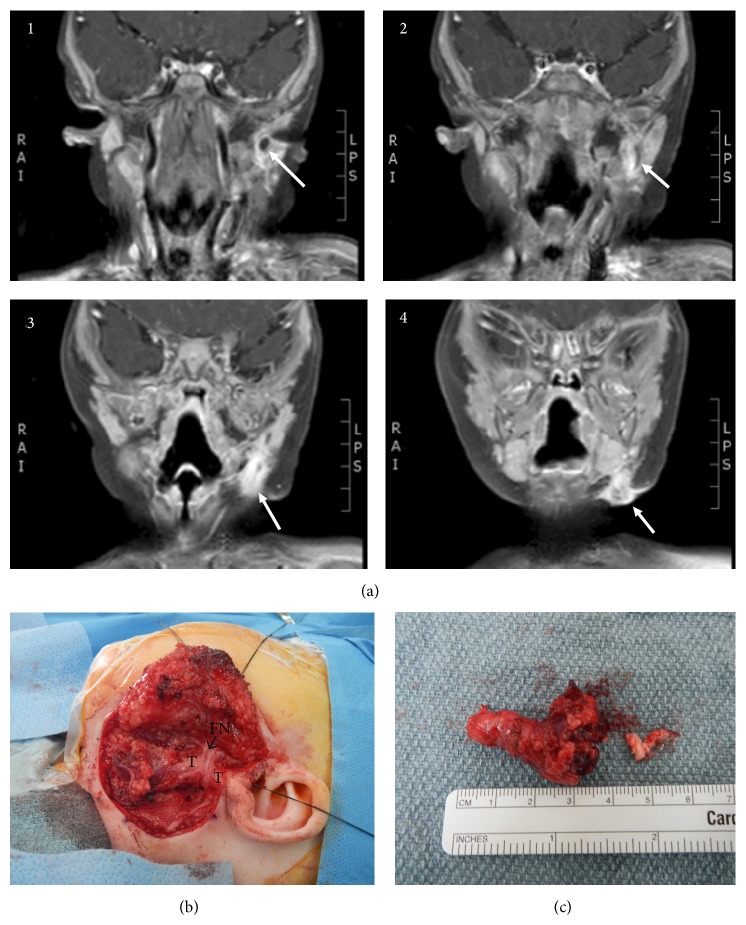
Objectives. First branchial cleft anomalies (BCAs) constitute a rare entity with variable clinical presentations and anatomic findings. Given the high rate of recurrence with incomplete excision, identification of the entire tract during surgical treatment is of paramount importance. The objectives of this paper were to present five anatomic variations of first BCAs and describe the presentation, evaluation, and surgical approach to each one. Methods. A retrospective case review and literature review were performed. We describe patient characteristics, presentation, evaluation, and surgical approach of five patients with first BCAs. Results. Age at definitive surgical treatment ranged from 8 months to 7 years. Various clinical presentations were encountered, some of which were atypical for first BCAs. All had preoperative imaging demonstrating the tract. Four surgical approaches required a superficial parotidectomy with identification of the facial nerve, one of which revealed an aberrant facial nerve. In one case the tract was found to travel into the angle of the mandible, terminating as a mandibular cyst. This required en bloc excision that included the lateral cortex of the mandible. Conclusions. First BCAs have variable presentations. Complete surgical excision can be challenging. Therefore, careful preoperative planning and the recognition of atypical variants during surgery are essential.
Figures




Similar articles
-
First branchial cleft anomalies in children: Experience with 30 cases.Exp Ther Med. 2017 Jul;14(1):333-337. doi: 10.3892/etm.2017.4511. Epub 2017 May 24. Exp Ther Med. 2017. PMID: 28672934 Free PMC article.
-
Branchial anomalies in children.Int J Pediatr Otorhinolaryngol. 2011 Aug;75(8):1020-3. doi: 10.1016/j.ijporl.2011.05.008. Epub 2011 Jun 15. Int J Pediatr Otorhinolaryngol. 2011. PMID: 21680029
-
Atypical first branchial cleft fistula: A case report.Int J Surg Case Rep. 2021 Jan;78:159-161. doi: 10.1016/j.ijscr.2020.12.007. Epub 2020 Dec 5. Int J Surg Case Rep. 2021. PMID: 33352445 Free PMC article.
-
Branchial cleft anomalies: a five-year retrospective review.Trans Pa Acad Ophthalmol Otolaryngol. 1990;42:1022-5. Trans Pa Acad Ophthalmol Otolaryngol. 1990. PMID: 2084977 Review.
-
Duplicated facial nerve trunk with a first branchial cleft cyst.Laryngoscope. 2014 Mar;124(3):662-4. doi: 10.1002/lary.24365. Epub 2013 Sep 19. Laryngoscope. 2014. PMID: 23946158 Review.
Cited by
-
New classification and surgical strategy for work type I congenital first branchial cleft anomalies in children.Eur Arch Otorhinolaryngol. 2023 Dec;280(12):5539-5546. doi: 10.1007/s00405-023-08140-4. Epub 2023 Jul 28. Eur Arch Otorhinolaryngol. 2023. PMID: 37505262
-
First branchial cleft anomalies in children: Experience with 30 cases.Exp Ther Med. 2017 Jul;14(1):333-337. doi: 10.3892/etm.2017.4511. Epub 2017 May 24. Exp Ther Med. 2017. PMID: 28672934 Free PMC article.
-
Perplexing First Branchialcleft Anomalies-A Case Series with Review of Literature.Indian J Otolaryngol Head Neck Surg. 2024 Feb;76(1):1454-1460. doi: 10.1007/s12070-023-04243-w. Epub 2023 Oct 7. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 38440503 Free PMC article.
-
Significance of the auditory meatus inferior wall cartilage in the surgical treatment of congenital first branchial cleft anomalies in children.World J Pediatr Surg. 2023 Nov 9;6(4):e000645. doi: 10.1136/wjps-2023-000645. eCollection 2023. World J Pediatr Surg. 2023. PMID: 38025903 Free PMC article.
-
First branchial cleft sinus with duplicate external auditory canal: A case report.Clin Case Rep. 2022 Apr 8;10(4):e05496. doi: 10.1002/ccr3.5496. eCollection 2022 Apr. Clin Case Rep. 2022. PMID: 35425605 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
