

Osmotherapy With Hypertonic Saline Attenuates Global Cerebral Edema Following Experimental Cardiac Arrest via Perivascular Pool of Aquaporin-4
- PMID: 27035238
- PMCID: PMC4949130
- DOI: 10.1097/CCM.0000000000001671
Osmotherapy With Hypertonic Saline Attenuates Global Cerebral Edema Following Experimental Cardiac Arrest via Perivascular Pool of Aquaporin-4
Abstract
Objectives: We tested the hypothesis that osmotherapy with hypertonic saline attenuates cerebral edema following experimental cardiac arrest and cardiopulmonary resuscitation by exerting its effect via the perivascular pool of aquaporin-4. We used mice with targeted disruption of the gene encoding α-syntrophin (α-Syn) that demonstrate diminished perivascular aquaporin-4 pool but retain the non-endfoot and ependymal pools.
Design: Laboratory animal study.
Setting: University animal research laboratory.
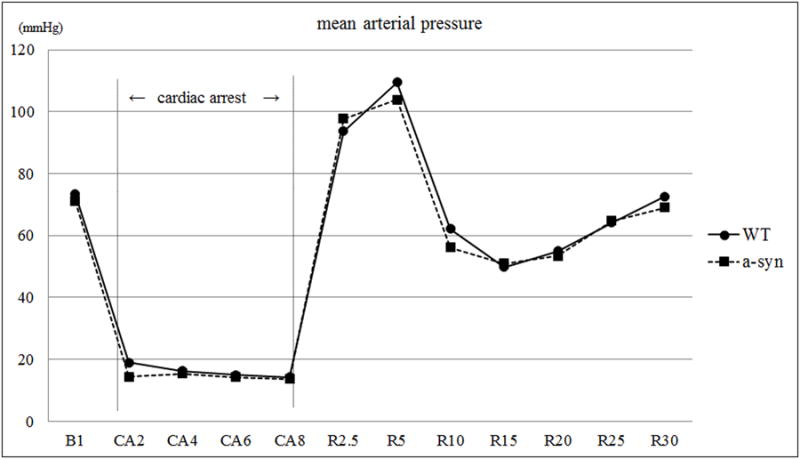
Interventions: Isoflurane-anesthetized adult male wild-type C57B/6 or α-Syn mice were subjected to cardiac arrest/cardiopulmonary resuscitation and treated with either a continuous IV infusion of 0.9% saline or various concentrations of hypertonic saline. Serum osmolality, regional brain water content, blood-brain barrier disruption, and aquaporin-4 protein expression were determined at 24 hours after cardiac arrest/cardiopulmonary resuscitation.
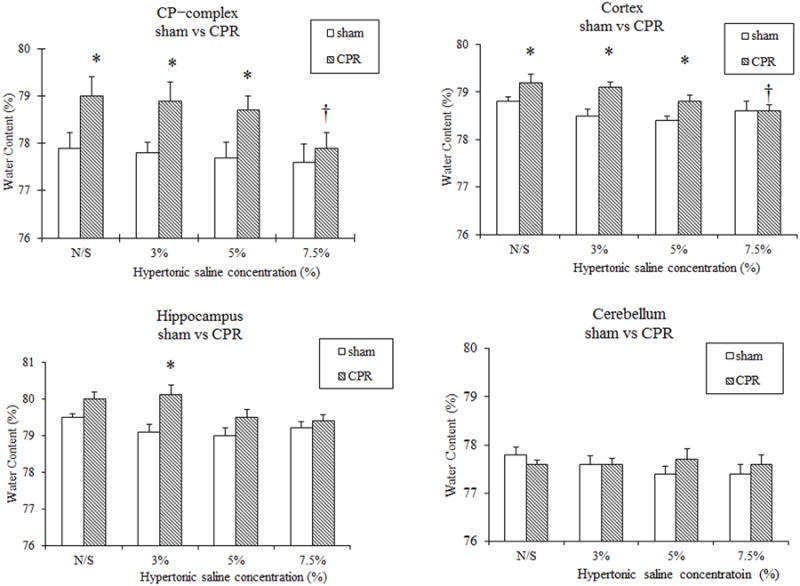
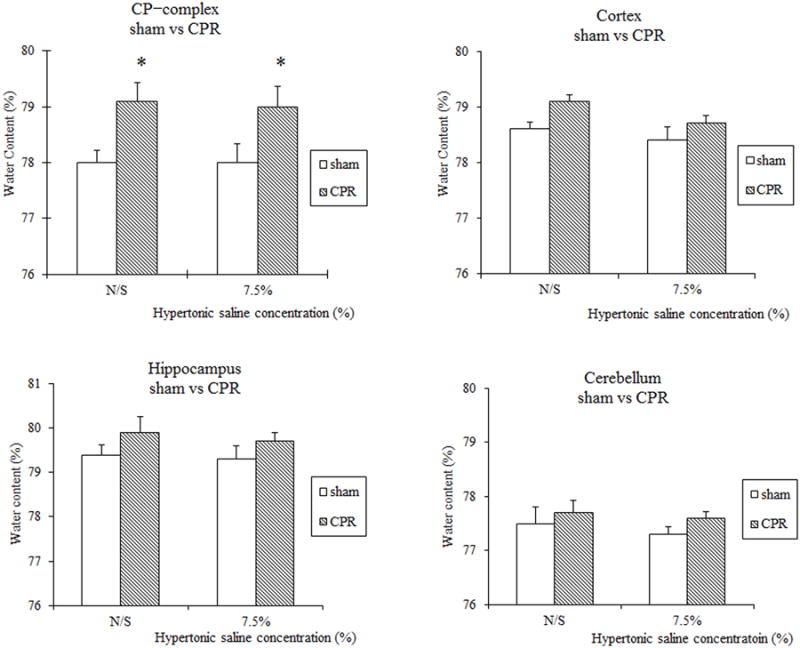
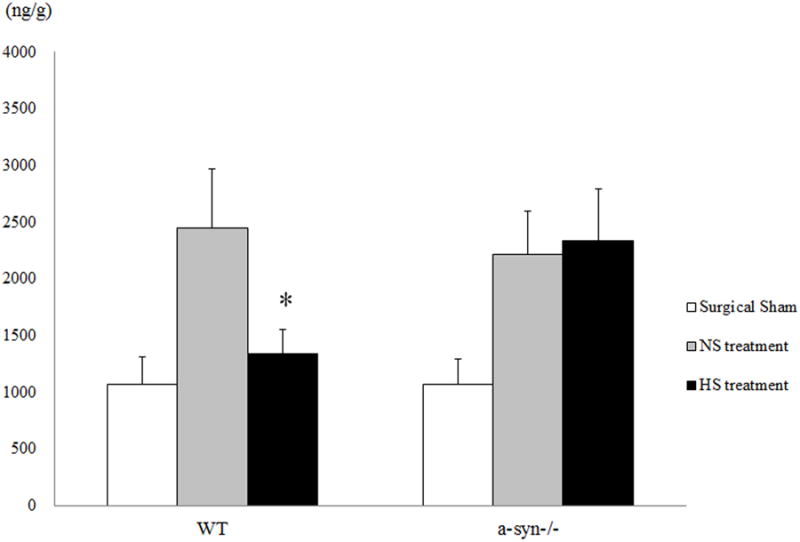
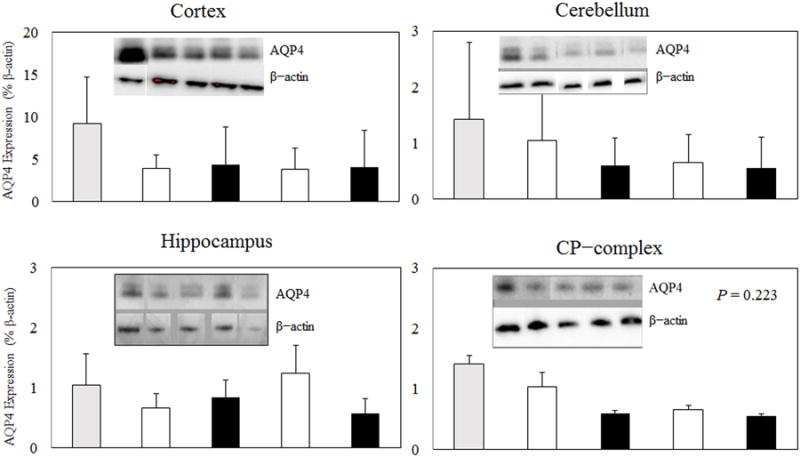
Measurements and main results: Hypertonic saline (7.5%) treatment significantly attenuated water content in the caudoputamen complex and cortex compared with 0.9% saline treatment in wild-type mice subjected to cardiac arrest/cardiopulmonary resuscitation. In contrast, in α-Syn mice subjected to cardiac arrest/cardiopulmonary resuscitation, 7.5% hypertonic saline treatment did not attenuate water content. Treatment with 7.5% hypertonic saline attenuated blood-brain barrier disruption at 24 hours following cardiac arrest/cardiopulmonary resuscitation in wild-type mice but not in α-Syn mice. Total aquaporin-4 protein expression was not different between 0.9% saline and hypertonic saline-treated wild-type mice.
Conclusions: Following experimental cardiac arrest/cardiopulmonary resuscitation: 1) continuous hypertonic saline therapy maintained to achieve serum osmolality of ≈ 350 mOsm/L is beneficial for the treatment of cerebral edema; 2) perivascular pool of aquaporin-4 plays a critical role in water egress from brain; and 3) hypertonic saline attenuates blood-brain barrier disruption via perivascular aquaporin-4 pool.
Conflict of interest statement
Figures
Similar articles
-
The perivascular pool of aquaporin-4 mediates the effect of osmotherapy in postischemic cerebral edema.Crit Care Med. 2008 Sep;36(9):2634-40. doi: 10.1097/CCM.0b013e3181847853. Crit Care Med. 2008. PMID: 18679106 Free PMC article.
-
Conivaptan, a Selective Arginine Vasopressin V1a and V2 Receptor Antagonist Attenuates Global Cerebral Edema Following Experimental Cardiac Arrest via Perivascular Pool of Aquaporin-4.Neurocrit Care. 2016 Apr;24(2):273-82. doi: 10.1007/s12028-015-0236-4. Neurocrit Care. 2016. PMID: 26732270
-
Increases in lung and brain water following experimental stroke: effect of mannitol and hypertonic saline.Crit Care Med. 2005 Jan;33(1):203-8; discussion 259-60. doi: 10.1097/01.ccm.0000150659.15558.23. Crit Care Med. 2005. PMID: 15644670
-
Anchoring of aquaporin-4 in brain: molecular mechanisms and implications for the physiology and pathophysiology of water transport.Neuroscience. 2004;129(4):999-1010. doi: 10.1016/j.neuroscience.2004.08.049. Neuroscience. 2004. PMID: 15561415 Review.
-
Bench to bedside: brain edema and cerebral resuscitation: the present and future.Acad Emerg Med. 2002 Sep;9(9):933-46. doi: 10.1111/j.1553-2712.2002.tb02196.x. Acad Emerg Med. 2002. PMID: 12208684 Review.
Cited by
-
Recovery among post-arrest patients with mild-to-moderate cerebral edema.Resuscitation. 2021 May;162:149-153. doi: 10.1016/j.resuscitation.2021.02.033. Epub 2021 Mar 1. Resuscitation. 2021. PMID: 33662524 Free PMC article.
-
Brain Hypoxia Is Associated With Neuroglial Injury in Humans Post-Cardiac Arrest.Circ Res. 2021 Aug 20;129(5):583-597. doi: 10.1161/CIRCRESAHA.121.319157. Epub 2021 Jul 21. Circ Res. 2021. PMID: 34287000 Free PMC article. Clinical Trial.
-
Deletion of aquaporin-4 improves capillary blood flow distribution in brain edema.Glia. 2023 Nov;71(11):2559-2572. doi: 10.1002/glia.24439. Epub 2023 Jul 13. Glia. 2023. PMID: 37439315 Free PMC article.
-
Emerging therapeutic targets for cerebral edema.Expert Opin Ther Targets. 2021 Nov;25(11):917-938. doi: 10.1080/14728222.2021.2010045. Epub 2022 Jan 2. Expert Opin Ther Targets. 2021. PMID: 34844502 Free PMC article. Review.
-
Oxygen administration in patients recovering from cardiac arrest: a narrative review.J Intensive Care. 2020 Aug 12;8:60. doi: 10.1186/s40560-020-00477-w. eCollection 2020. J Intensive Care. 2020. PMID: 32832091 Free PMC article. Review.
References
-
- Stiell IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):647–656. - PubMed
-
- Vaillancourt C, Stiell IG Canadian Cardiovascular Outcomes Research T. Cardiac arrest care and emergency medical services in Canada. Can J Cardiol. 2004;20(11):1081–1090. - PubMed
-
- Richmond TS. Cerebral resuscitation after global brain ischemia: linking research to practice. AACN Clin Issues. 1997;8(2):171–181. - PubMed
-
- White BC, Sullivan JM, DeGracia DJ, et al. Brain ischemia and reperfusion: molecular mechanisms of neuronal injury. J Neurol Sci. 2000;179(S 1-2):1–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
