

Development of an algorithm to aid triage decisions for intensive care unit admission: a clinical vignette and retrospective cohort study
- PMID: 27036102
- PMCID: PMC4818478
- DOI: 10.1186/s13054-016-1262-0
Development of an algorithm to aid triage decisions for intensive care unit admission: a clinical vignette and retrospective cohort study
Abstract
Background: Intensive care unit (ICU) admission triage is performed routinely and is often based solely on clinical judgment, which could mask biases. A computerized algorithm to aid ICU triage decisions was developed to classify patients into the Society of Critical Care Medicine's prioritization system. In this study, we sought to evaluate the reliability and validity of this algorithm.
Methods: Nine senior physicians evaluated forty clinical vignettes based on real patients. The reference standard was defined as the priorities ascribed by two investigators with full access to patients' records. Agreement of algorithm-based priorities with the reference standard and with intuitive priorities provided by the physicians were evaluated. Correlations between algorithm prioritization and physicians' judgment of the appropriateness of ICU admissions in scarcity and nonscarcity settings were also evaluated. Validity was further assessed by retrospectively applying this algorithm to 603 patients with requests for ICU admission for association with clinical outcomes.
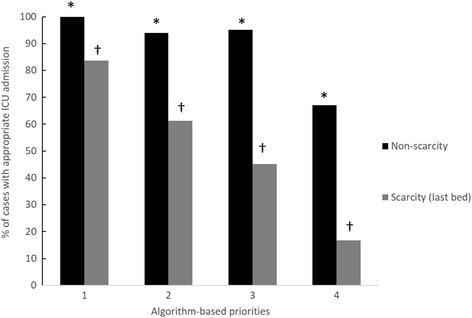
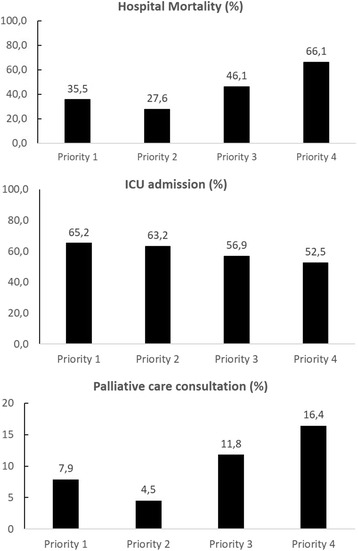
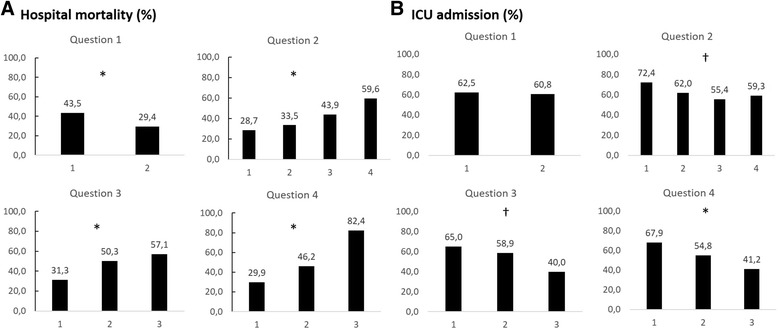
Results: Agreement between algorithm-based priorities and the reference standard was substantial, with a median κ of 0.72 (interquartile range [IQR] 0.52-0.77). Algorithm-based priorities demonstrated higher interrater reliability (overall κ 0.61, 95% confidence interval [CI] 0.57-0.65; median percentage agreement 0.64, IQR 0.59-0.70) than physicians' intuitive prioritization (overall κ 0.51, 95% CI 0.47-0.55; median percentage agreement 0.49, IQR 0.44-0.56) (p = 0.001). Algorithm-based priorities were also associated with physicians' judgment of appropriateness of ICU admission (priorities 1, 2, 3, and 4 vignettes would be admitted to the last ICU bed in 83.7%, 61.2%, 45.2%, and 16.8% of the scenarios, respectively; p < 0.001) and with actual ICU admission, palliative care consultation, and hospital mortality in the retrospective cohort.
Conclusions: This ICU admission triage algorithm demonstrated good reliability and validity. However, more studies are needed to evaluate a difference in benefit of ICU admission justifying the admission of one priority stratum over the others.
Figures
Similar articles
-
The Perceived Likelihood of Outcome of Critical Care Patients and Its Impact on Triage Decisions: A Case-Based Survey of Intensivists and Internists in a Canadian, Quaternary Care Hospital Network.PLoS One. 2016 Feb 12;11(2):e0149196. doi: 10.1371/journal.pone.0149196. eCollection 2016. PLoS One. 2016. PMID: 26871587 Free PMC article.
-
Prospective evaluation of patients refused admission to an intensive care unit: triage, futility and outcome.Intensive Care Med. 2001 Sep;27(9):1459-65. doi: 10.1007/s001340101041. Intensive Care Med. 2001. PMID: 11685338
-
A decision-aid tool for ICU admission triage is associated with a reduction in potentially inappropriate intensive care unit admissions.J Crit Care. 2019 Jun;51:77-83. doi: 10.1016/j.jcrc.2019.02.002. Epub 2019 Feb 4. J Crit Care. 2019. PMID: 30769294
-
The Critical Care Society of Southern Africa Consensus Guideline on ICU Triage and Rationing (ConICTri).S Afr Med J. 2019 Aug 22;109(8b):630-642. doi: 10.7196/SAMJ.2019.v109i8b.13. S Afr Med J. 2019. PMID: 31456541
-
Critically ill cancer patient in intensive care unit: issues that arise.J Crit Care. 2014 Oct;29(5):817-22. doi: 10.1016/j.jcrc.2014.04.007. Epub 2014 Apr 24. J Crit Care. 2014. PMID: 24857640 Review.
Cited by
-
Evaluation of bed vacancy and occupancy times as governance parameters in patients admitted to a public intensive care unit.Rev Bras Ter Intensiva. 2020 Jul-Sep;32(3):412-417. doi: 10.5935/0103-507X.20200070. Rev Bras Ter Intensiva. 2020. PMID: 33053031 Free PMC article.
-
Factors potentially associated with the decision of admission to the intensive care unit in a middle-income country: a survey of Brazilian physicians.Rev Bras Ter Intensiva. 2017 Apr-Jun;29(2):154-162. doi: 10.5935/0103-507X.20170025. Rev Bras Ter Intensiva. 2017. PMID: 28977256 Free PMC article.
-
Optimal age- and sex-based management of the queue to ventilators during the Covid-19 crisis.J Math Econ. 2021 Mar;93:102494. doi: 10.1016/j.jmateco.2021.102494. Epub 2021 Feb 11. J Math Econ. 2021. PMID: 33594295 Free PMC article.
-
Impact of nonclinical factors on intensive care unit admission decisions: a vignette-based randomized trial (V-TRIAGE).Rev Bras Ter Intensiva. 2021 Apr-Jun;33(2):219-230. doi: 10.5935/0103-507X.20210029. Rev Bras Ter Intensiva. 2021. PMID: 34231802 Free PMC article. Clinical Trial.
-
The Influential Factor Analysis of Classification Partition Management Mode on the Emergency Triage.Iran J Public Health. 2016 Jul;45(7):885-9. Iran J Public Health. 2016. PMID: 27516994 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
