

Prevalence, awareness, treatment, control and risk factors related to hypertension among urban adults in Inner Mongolia 2014: differences between Mongolian and Han populations
- PMID: 27036609
- PMCID: PMC4818445
- DOI: 10.1186/s12889-016-2965-5
Prevalence, awareness, treatment, control and risk factors related to hypertension among urban adults in Inner Mongolia 2014: differences between Mongolian and Han populations
Abstract
Background: Han and Mongolian populations constitute approximately 96% of the population of Inner Mongolia Autonomous Region, and the two ethnic groups have different genetic backgrounds and lifestyle. We aim to assess the prevalence, awareness, treatment, control, and related risk factors of hypertension among urban adults in Inner Mongolia, with the comparison of the differences between Mongolian and Han populations in this respect.
Methods: Three thousand two hundred fifty-one individuals aged 20-80 years (2326 Han and 925 Mongolian) were selected using a multistage cluster sampling method from Inner Mongolia in 2014. The adjusted prevalence, awareness, treatment and control of hypertension were evaluated by the Logistic regression. In addition, possible interactions were also tested. When interactions were found significant, strata-specific analysis were performed. Multivariate logistic regression was used for estimating independent associations between risk factors and hypertension.
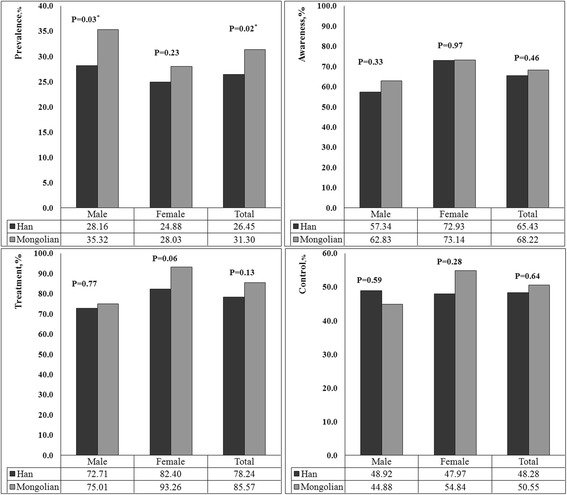
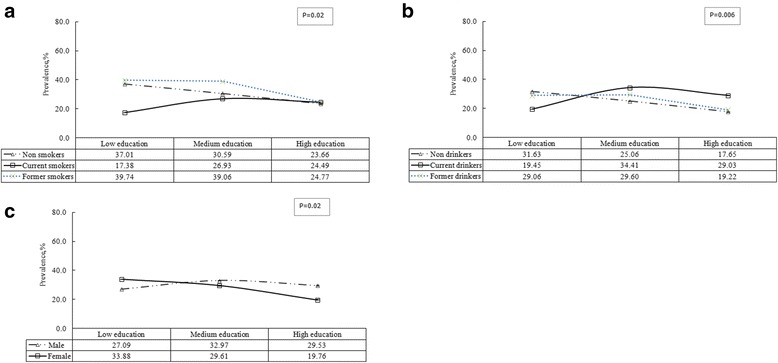
Results: The prevalence of hypertension was 27.47% for Han population, 31.46% for Mongolian population. The adjusted prevalence, awareness, treatment and control of hypertension were 26.45, 65.43, 78.24 and 48.28% in Han, and 31.30, 68.22, 85.57 and 50.55% in Mongolian, respectively. There was no significant difference in the adjusted awareness, treatment and control of hypertension among Mongolian and Han adult residents (all P >0.05). Lower prevalence of hypertension was associated with younger age and healthy weight in both Mongolian and Han adults. Within Han adults, high education, moderate physical activity and non-alcohol drinkers were additionally associated with lower prevalence of hypertension, whereas within Mongolian adults, lower prevalence was associated with being female. Among residents with medium education level, nondrinkers had 0.60 times lower odds of having hypertension than current drinkers (OR = 0.60, 95% CI: 0.44-0.82); among residents with high education level, nondrinkers has 0.65 times lower odds of having hypertension than current drinkers (OR = 0.65, 95% CI: 0.43-0.97).
Conclusions: Mongolian population had a higher prevalence of hypertension than Han population. There were no significant difference between Mongolian and Han population in awareness, treatment and control of hypertension, which suggested that there was no difference between the two ethnicities in the distribution of health resources.
Keywords: Ethnicity; Han; Hypertension; Mongolian; Urban.
Figures
Similar articles
-
Prevalence of and risk factors for refractive error: a cross-sectional study in Han and Mongolian adults aged 40-80 years in Inner Mongolia, China.Eye (Lond). 2019 Nov;33(11):1722-1732. doi: 10.1038/s41433-019-0469-0. Epub 2019 Jun 3. Eye (Lond). 2019. PMID: 31160702 Free PMC article.
-
[Prevalence, detection, management, and control of hypertension in the population of Mongolian and Han nationalities with age ≥ 55 years in a pastoral area of Inner Mongolia Autonomous Region].Zhonghua Xin Xue Guan Bing Za Zhi. 2012 Sep;40(9):786-90. Zhonghua Xin Xue Guan Bing Za Zhi. 2012. PMID: 23141094 Chinese.
-
Association of prehypertension and cardiovascular risk factor clustering in Inner Mongolia: a cross-sectional study.BMJ Open. 2017 Jun 30;7(6):e015340. doi: 10.1136/bmjopen-2016-015340. BMJ Open. 2017. PMID: 28667215 Free PMC article.
-
Hypertension awareness, treatment and control among ethnic minority populations in Europe: a systematic review and meta-analysis.J Hypertens. 2021 Feb 1;39(2):202-213. doi: 10.1097/HJH.0000000000002651. J Hypertens. 2021. PMID: 32925300 Free PMC article.
-
Hypertension in a multi-ethnic Asian population of Singapore.J Clin Hypertens (Greenwich). 2021 Mar;23(3):522-528. doi: 10.1111/jch.14140. Epub 2020 Dec 19. J Clin Hypertens (Greenwich). 2021. PMID: 33340436 Free PMC article. Review.
Cited by
-
Diet quality is associated with reduced risk of hypertension among Inner Mongolia adults in northern China.Public Health Nutr. 2020 Jun;23(9):1543-1554. doi: 10.1017/S136898001900301X. Epub 2019 Nov 5. Public Health Nutr. 2020. PMID: 31685051 Free PMC article.
-
Prevalence and risk factors of prehypertension/hypertension among freshman students from the Vietnam National University: a cross-sectional study.BMC Public Health. 2023 Jun 16;23(1):1166. doi: 10.1186/s12889-023-16118-4. BMC Public Health. 2023. PMID: 37328903 Free PMC article.
-
Protocol of the Inner Mongolian Healthy Aging Study (IMAGINS): a longitudinal cohort study.BMC Public Health. 2022 Jan 17;22(1):115. doi: 10.1186/s12889-022-12542-0. BMC Public Health. 2022. PMID: 35039022 Free PMC article.
-
Prevalence of and risk factors for refractive error: a cross-sectional study in Han and Mongolian adults aged 40-80 years in Inner Mongolia, China.Eye (Lond). 2019 Nov;33(11):1722-1732. doi: 10.1038/s41433-019-0469-0. Epub 2019 Jun 3. Eye (Lond). 2019. PMID: 31160702 Free PMC article.
-
Prevalence and Risk Factors of Prehypertension and Hypertension in Southern China.PLoS One. 2017 Jan 17;12(1):e0170238. doi: 10.1371/journal.pone.0170238. eCollection 2017. PLoS One. 2017. PMID: 28095471 Free PMC article.
References
-
- Hu SS, Kong LZ, Gao RL, Zhu ML, Wang W, Wang YJ, Wu ZS, Chen WW, Liu MB. Outline of the report on cardiovascular disease in China, 2010. Biomed Environ Sci. 2012;25(3):251–256. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
