

Long-term outcomes and healthcare utilization following critical illness--a population-based study
- PMID: 27037030
- PMCID: PMC4818427
- DOI: 10.1186/s13054-016-1248-y
Long-term outcomes and healthcare utilization following critical illness--a population-based study
Abstract
Background: The purpose of this study was to examine hospital mortality, long-term mortality, and health service utilization among critically ill patients. We also determined whether these outcomes differed according to demographic and clinical characteristics.
Methods: We conducted a retrospective cohort study of adults (age ≥ 18 years) who survived admission to an intensive care unit (ICU) in Ontario, Canada, between 1 April 2002 and 31 March 2012, excluding isolated admissions to step-down or intermediate ICUs, coronary care ICUs, or cardiac surgery ICUs. Adults (age ≥ 18 years) who survived an acute hospitalization that did not include an ICU stay formed the comparator group. The primary outcome was mortality following hospital discharge. Secondary outcomes were healthcare utilization, including emergency room admissions and hospital readmissions during follow-up.
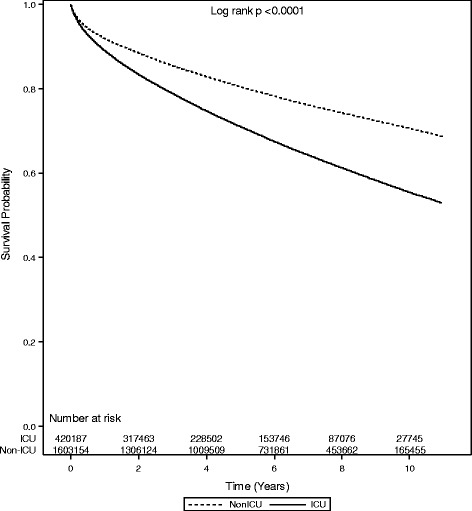
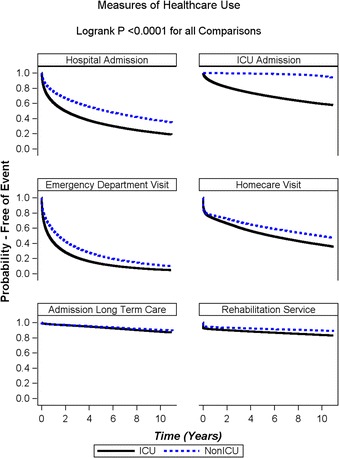
Results: Over the study interval, 500,124 patients were admitted to ICUs and 420,187 (84%) survived to hospital discharge. Median follow-up for survivors was 5.3 (interquartile range 2.5, 8.2) years. Patients admitted to an ICU were more likely to subsequently visit the emergency department, be readmitted to the hospital and ICU, receive home care support, require rehabilitation, and be admitted for long-term care. Those requiring more resources within the ICU required more resources after discharge. One-third of patients admitted to the ICU died during long-term follow-up, with overall probabilities of death of 11% and 29% at 1 year and 5 years, respectively. In the adjusted analysis, there was an increasing hazard of death with increasing age, reaching a hazard ratio of 18.08 (95 % confidence interval 16.60-19.68) for those ≥ 85 years of age compared with those aged 18-24 years.
Conclusions: Healthcare utilization after hospital discharge was higher among ICU patients, and also among those requiring more healthcare resources during their ICU admission, than among all hospitalized patients as a group. One-third of ICU patients died within the 5 years following discharge, and age was the most influential determinant of outcome. These findings should help target post-ICU discharge services for high-risk groups and better inform goals-of-care discussions for elderly critically ill patients.
Keywords: Critical care; Healthcare utilization; Outcomes.
Figures
Similar articles
-
A population-based observational study of intensive care unit-related outcomes. With emphasis on post-hospital outcomes.Ann Am Thorac Soc. 2015 Feb;12(2):202-8. doi: 10.1513/AnnalsATS.201405-201CME. Ann Am Thorac Soc. 2015. PMID: 25706486
-
Increased risk of death and readmission after hospital discharge of critically ill patients in a developing country: a retrospective multicenter cohort study.Intensive Care Med. 2018 Jul;44(7):1090-1096. doi: 10.1007/s00134-018-5252-3. Epub 2018 Jul 12. Intensive Care Med. 2018. PMID: 30003303
-
The association of acute kidney injury in the critically ill and postdischarge outcomes: a cohort study*.Crit Care Med. 2015 Feb;43(2):354-64. doi: 10.1097/CCM.0000000000000706. Crit Care Med. 2015. PMID: 25474534
-
Survival, Quality of Life, and Functional Status Following Prolonged ICU Stay in Cardiac Surgical Patients: A Systematic Review.Crit Care Med. 2019 Jan;47(1):e52-e63. doi: 10.1097/CCM.0000000000003504. Crit Care Med. 2019. PMID: 30398978
-
[When is the intensive care patient ready for discharge?].Lakartidningen. 2002 Mar 27;99(13):1432-4. Lakartidningen. 2002. PMID: 11989350 Review. Swedish.
Cited by
-
Challenges in conducting long-term outcomes studies in critical care.Curr Opin Crit Care. 2019 Oct;25(5):473-488. doi: 10.1097/MCC.0000000000000650. Curr Opin Crit Care. 2019. PMID: 31356238 Free PMC article. Review.
-
Qualitative, grounded theory exploration of patients' experience of early mobilisation, rehabilitation and recovery after critical illness.BMJ Open. 2019 Feb 24;9(2):e026348. doi: 10.1136/bmjopen-2018-026348. BMJ Open. 2019. PMID: 30804034 Free PMC article.
-
The performance of acute versus antecedent patient characteristics for 1-year mortality prediction during intensive care unit admission: a national cohort study.Crit Care. 2020 Jun 11;24(1):330. doi: 10.1186/s13054-020-03017-y. Crit Care. 2020. PMID: 32527298 Free PMC article.
-
Exploring the impact of arginine-supplemented immunonutrition on length of stay in the intensive care unit: A retrospective cross-sectional analysis.PLoS One. 2024 Apr 26;19(4):e0302074. doi: 10.1371/journal.pone.0302074. eCollection 2024. PLoS One. 2024. PMID: 38669262 Free PMC article.
-
Effect of Inpatient Pharmacist-Led Medication Reconciliations on Medication-Related Interventions in Intensive Care Unit Recovery Centers.Hosp Pharm. 2024 Dec;59(6):650-659. doi: 10.1177/00185787241269113. Epub 2024 Aug 7. Hosp Pharm. 2024. PMID: 39493571
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
