

Treatment of periprosthetic acetabular fractures after previous hemi- or total hip arthroplasty: Introduction of a new implant
- PMID: 27037805
- PMCID: PMC4823337
- DOI: 10.1007/s00064-016-0439-7
Treatment of periprosthetic acetabular fractures after previous hemi- or total hip arthroplasty: Introduction of a new implant
Abstract
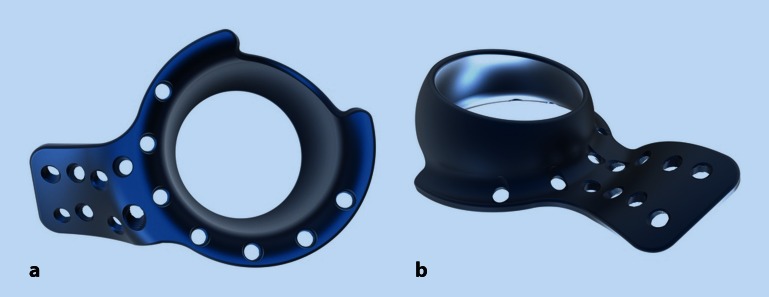
Objective: Treatment of displaced periprosthetic acetabular fractures in elderly patients. The goal is to stabilize an acetabular fracture independent of the fracture pattern, by inserting the custom-made roof-reinforcement plate and starting early postoperative full weight-bearing mobilization.
Indications: Acetabular fracture with or without previous hemi- or total hip arthroplasty.
Contraindications: Non-displaced acetabular fractures.
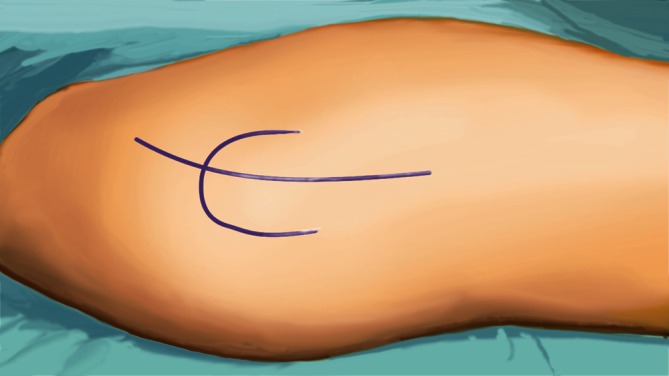
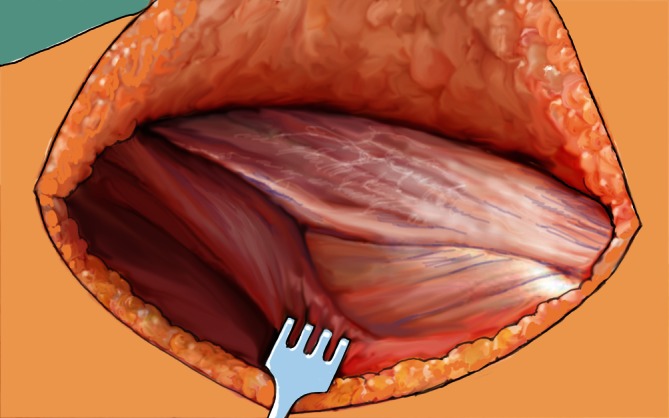
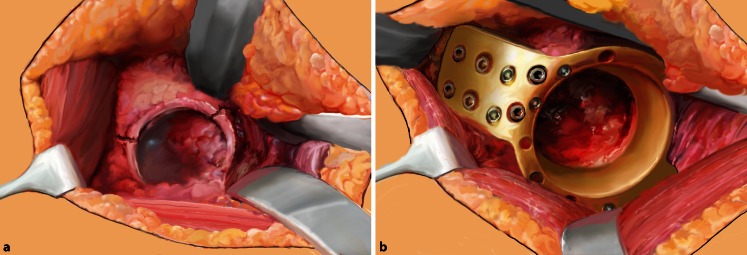
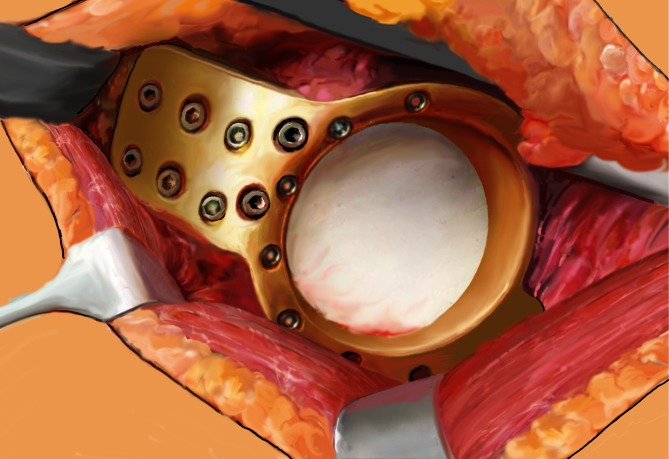
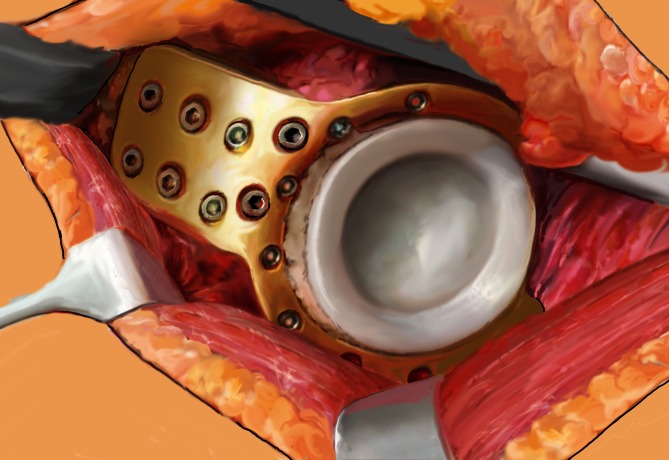
Surgical technique: Watson-Jones approach to provide accessibility to the anterior and supraacetabular part of the iliac bone. Angle-stable positioning of the roof-reinforcement plate without any fracture reduction. Cementing a polyethylene cup into the metal plate and restoring prosthetic femoral components.
Postoperative management: Full weight-bearing mobilization within the first 10 days after surgery. In cases of two column fractures, partial weight-bearing is recommended.
Results: Of 7 patients with periprosthetic acetabular fracture, 5 were available for follow-up at 3, 6, 6, 15, and 24 months postoperatively. No complications were recognized and all fractures showed bony consolidation. Early postoperative mobilization was started within the first 10 days. All patients except one reached their preinjury mobility level. This individual and novel implant is custom made for displaced acetabular and periprosthetic fractures in patients with osteopenic bone. It provides a hopeful benefit due to early full weight-bearing mobilization within the first 10 days after surgery.
Limitations: In case of largely destroyed supraacetabular bone or two-column fractures according to Letournel additional synthesis via an anterior approach might be necessary. In these cases partial weight bearing is recommended.
Operationsziel: Ziel ist die Behandlung von dislozierten periprothetischen Azetabulumfrakturen bei älteren Patienten. Dabei werden Frakturen des Azetabulums unabhängig vom Frakturmuster durch Einsetzen einer sonderangefertigten Azetabulumabstützpfanne stabilisiert und eine frühe postoperative Mobilisation unter Vollbelastung begonnen.
Indikationen: Azetabulumfraktur mit oder ohne vorherige Hüftendoprothetik.
Kontraindikationen: Nichtdislozierte Azetabulumfrakturen.
Operationstechnik: Zugang nach Watson-Jones, um die Erreichbarkeit des vorderen und supraazetabulären Anteils des Darmbeins zu ermöglichen. Winkelstabile Positionierung der Azetabulumabstützpfanne ohne Frakturreposition. Zementieren einer Polyethylenpfanne in die Metallplatte und Reposition der femoralen Prothesenkomponenten.
Weiterbehandlung: Mobilisation unter Vollbelastung innerhalb der ersten 10 Tage nach Operation. In Fällen einer 2‑Pfeiler-Fraktur mit ungenügender Schraubenzahl im stabilen Knochen wird eine Teilbelastung empfohlen.
Ergebnisse: Von insgesamt 7 Fällen mit periprothetischer Azetabulumfraktur konnten 5 Patienten 3, 6, 6, 15 und 24 Monate postoperativ nachuntersucht werden. Es gab keine nennenswerten Komplikationen. Alle Frakturen zeigten eine knöcherne Konsolidierung. Eine frühe postoperative Mobilisation wurde in den ersten 10 Tagen begonnen und alle Patienten außer einem erreichten ihren ursprünglichen Mobilitätsgrad.
Schlussfolgerung: Dieses individuelle, neuartige Implantat ist für dislozierte Azetabulumfrakturen und periprothetische Frakturen bei Patienten mit osteoporotischem Knochen entwickelt worden. Es verspricht hoffnungsvollen Benefit aufgrund der frühen Vollmobilisation innerhalb der ersten 10 Tage nach Operation.
Einschränkungen: Bei stark zerstörten supraazetabulären Knochen- oder 2-Pfeiler-Frakturen nach Letournel könnte eine zusätzliche Synthese über einen anterioren Zugang notwendig sein. In diesen Fällen wird eine Teilbelastung empfohlen.
Keywords: Acetabulum; Mobilization; Osteoporosis; Prosthesis; Weight-bearing.
Figures


References
-
- McElfresh EC, Coventry MB. Femoral and pelvic fractures after total hip arthroplasty. J Bone Joint Surg Am. 1974;56(3):483–492. - PubMed
-
- Miller AJ. Late fracture of the acetabulum after total hip replacement. J Bone Joint Surg Br. 1972;54(4):600–606. - PubMed
-
- Silvello L, Scarponi R, Lucia G, Guazzetti R. Traumatic loosening of a prosthetic acetabular cup in a young patient. Ital J Orthop Traumatol. 1985;11(2):237–239. - PubMed
-
- Ochs BG, Marintschev I, Hoyer H, Rolauffs B, Culemann U, Pohlemann T, et al. Changes in the treatment of acetabular fractures over 15 years: Analysis of 1266 cases treated by the German Pelvic Multicentre Study Group (DAO/DGU) Injury. 2010;41(8):839–851. doi: 10.1016/j.injury.2010.04.010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
