

Corticosteroid therapy in refractory shock following cardiac arrest: a randomized, double-blind, placebo-controlled, trial
- PMID: 27038920
- PMCID: PMC4818959
- DOI: 10.1186/s13054-016-1257-x
Corticosteroid therapy in refractory shock following cardiac arrest: a randomized, double-blind, placebo-controlled, trial
Abstract
Background: The purpose of this study was to determine whether the provision of corticosteroids improves time to shock reversal and outcomes in patients with post-cardiac arrest shock.
Methods: We conducted a randomized, double-blind trial of post-cardiac arrest patients in shock, defined as vasopressor support for a minimum of 1 hour. Patients were randomized to intravenous hydrocortisone 100 mg or placebo every 8 hours for 7 days or until shock reversal. The primary endpoint was time to shock reversal.
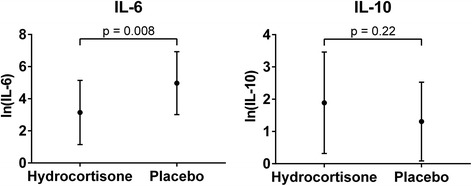
Results: Fifty patients were included with 25 in each group. There was no difference in time to shock reversal between groups (hazard ratio: 0.83 [95% CI: 0.40-1.75], p = 0.63). We found no difference in secondary outcomes including shock reversal (52% vs. 60%, p = 0.57), good neurological outcome (24% vs. 32%, p = 0.53) or survival to discharge (28% vs. 36%, p = 0.54) between the hydrocortisone and placebo groups. Of the patients with a baseline cortisol < 15 ug/dL, 100% (6/6) in the hydrocortisone group achieved shock reversal compared to 33% (1/3) in the placebo group (p = 0.08). All patients in the placebo group died (100%; 3/3) whereas 50% (3/6) died in the hydrocortisone group (p = 0.43).
Conclusions: In a population of cardiac arrest patients with vasopressor-dependent shock, treatment with hydrocortisone did not improve time to shock reversal, rate of shock reversal, or clinical outcomes when compared to placebo.
Clinical trial registration: Clinicaltrials.gov: NCT00676585, registration date: May 9, 2008.
Keywords: Adrenal; Cardiac arrest; Hydrocortisone; Shock; Steroids; Vasopressors.
Figures
Comment in
-
Surrogate endpoints and competing risk of death in cardiac arrest research.Crit Care. 2016 Jun 29;20(1):189. doi: 10.1186/s13054-016-1345-y. Crit Care. 2016. PMID: 27353499 Free PMC article.
-
Possible significance of hemodynamic and immunomodulatory effects of early stress-dose steroids in cardiac arrest.Crit Care. 2016 Jul 20;20(1):211. doi: 10.1186/s13054-016-1384-4. Crit Care. 2016. PMID: 27436285 Free PMC article. No abstract available.
References
-
- Field JM, Hazinski MF, Sayre MR, Chameides L, Schexnayder SM, Hemphill R, et al. Part 1: executive summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S640–56. doi: 10.1161/CIRCULATIONAHA.110.970889. - DOI - PubMed
-
- International Liaison Committee on Resuscitation 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 4: Advanced life support. Resuscitation. 2005;67(2-3):213–47. doi: 10.1016/j.resuscitation.2005.09.018. - DOI - PubMed
-
- Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S768–86. doi: 10.1161/CIRCULATIONAHA.110.971002. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
