

The standard of care of patients with ARDS: ventilatory settings and rescue therapies for refractory hypoxemia
- PMID: 27040102
- PMCID: PMC4828494
- DOI: 10.1007/s00134-016-4325-4
The standard of care of patients with ARDS: ventilatory settings and rescue therapies for refractory hypoxemia
Abstract
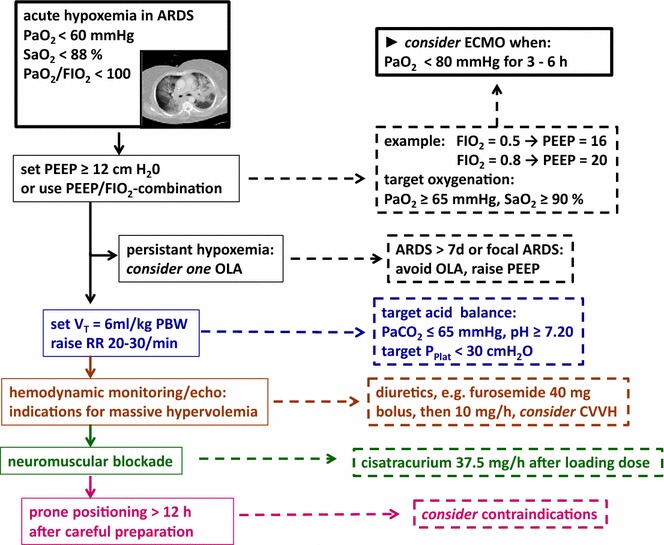
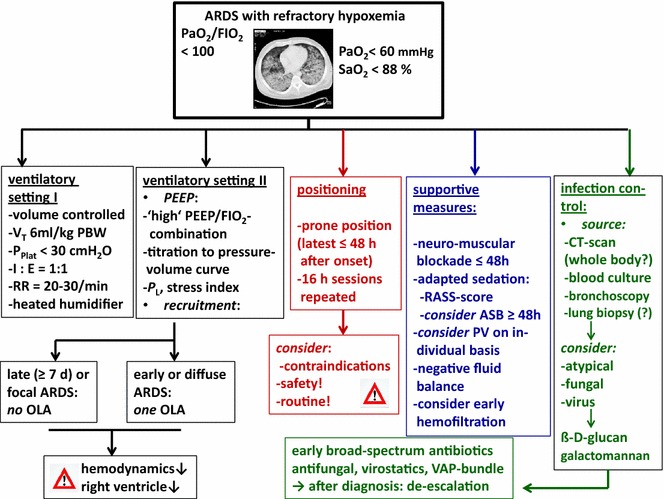
Purpose: Severe ARDS is often associated with refractory hypoxemia, and early identification and treatment of hypoxemia is mandatory. For the management of severe ARDS ventilator settings, positioning therapy, infection control, and supportive measures are essential to improve survival.
Methods and results: A precise definition of life-threating hypoxemia is not identified. Typical clinical determinations are: arterial partial pressure of oxygen < 60 mmHg and/or arterial oxygenation < 88 % and/or the ratio of PaO2/FIO2 < 100. For mechanical ventilation specific settings are recommended: limitation of tidal volume (6 ml/kg predicted body weight), adequate high PEEP (>12 cmH2O), a recruitment manoeuvre in special situations, and a 'balanced' respiratory rate (20-30/min). Individual bedside methods to guide PEEP/recruitment (e.g., transpulmonary pressure) are not (yet) available. Prone positioning [early (≤ 48 hrs after onset of severe ARDS) and prolonged (repetition of 16-hr-sessions)] improves survival. An advanced infection management/control includes early diagnosis of bacterial, atypical, viral and fungal specimen (blood culture, bronchoalveolar lavage), and of infection sources by CT scan, followed by administration of broad-spectrum anti-infectives. Neuromuscular blockage (Cisatracurium ≤ 48 hrs after onset of ARDS), as well as an adequate sedation strategy (score guided) is an important supportive therapy. A negative fluid balance is associated with improved lung function and the use of hemofiltration might be indicated for specific indications.
Conclusions: A specific standard of care is required for the management of severe ARDS with refractory hypoxemia.
Keywords: Acute respiratory distress syndrome; Infection management; Neuromuscular blockade; Prone positioning; Refractory hypoxemia; Ventilatory settings.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
References
-
- Abdelsalam M, Cheifetz IM. Goal-directed therapy for severely hypoxic patients with acute respiratory distress syndrome: permissive hypoxemia. Respir Care. 2010;55:1483–1490. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
