

Risk stratification of childhood medulloblastoma in the molecular era: the current consensus
- PMID: 27040285
- PMCID: PMC4867119
- DOI: 10.1007/s00401-016-1569-6
Risk stratification of childhood medulloblastoma in the molecular era: the current consensus
Abstract
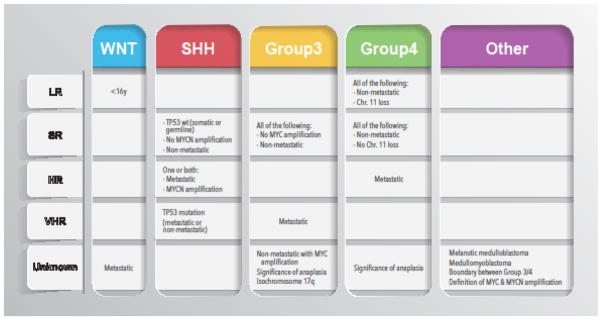
Historical risk stratification criteria for medulloblastoma rely primarily on clinicopathological variables pertaining to age, presence of metastases, extent of resection, histological subtypes and in some instances individual genetic aberrations such as MYC and MYCN amplification. In 2010, an international panel of experts established consensus defining four main subgroups of medulloblastoma (WNT, SHH, Group 3 and Group 4) delineated by transcriptional profiling. This has led to the current generation of biomarker-driven clinical trials assigning WNT tumors to a favorable prognosis group in addition to clinicopathological criteria including MYC and MYCN gene amplifications. However, outcome prediction of non-WNT subgroups is a challenge due to inconsistent survival reports. In 2015, a consensus conference was convened in Heidelberg with the objective to further refine the risk stratification in the context of subgroups and agree on a definition of risk groups of non-infant, childhood medulloblastoma (ages 3-17). Published and unpublished data over the past 5 years were reviewed, and a consensus was reached regarding the level of evidence for currently available biomarkers. The following risk groups were defined based on current survival rates: low risk (>90 % survival), average (standard) risk (75-90 % survival), high risk (50-75 % survival) and very high risk (<50 % survival) disease. The WNT subgroup and non-metastatic Group 4 tumors with whole chromosome 11 loss or whole chromosome 17 gain were recognized as low-risk tumors that may qualify for reduced therapy. High-risk strata were defined as patients with metastatic SHH or Group 4 tumors, or MYCN-amplified SHH medulloblastomas. Very high-risk patients are Group 3 with metastases or SHH with TP53 mutation. In addition, a number of consensus points were reached that should be standardized across future clinical trials. Although we anticipate new data will emerge from currently ongoing and recently completed clinical trials, this consensus can serve as an outline for prioritization of certain molecular subsets of tumors to define and validate risk groups as a basis for future clinical trials.
Keywords: Genomics; Group 3; Group 4; Medulloblastoma; Outcomes; SHH; Subgroups; WNT; p53.
Figures
References
-
- Bull KS, Spoudeas HA, Yadegarfar G, Kennedy CR. Reduction of health status 7 years after addition of chemotherapy to craniospinal irradiation for medulloblastoma: a follow-up study in PNET 3 trial survivors on behalf of the CCLG (formerly UKCCSG) J Clin Oncol. 2007;25:4239–4245. doi: 10.1200/jco.2006.08.7684. - DOI - PubMed
-
- Camara-Costa H, Resch A, Kieffer V, Lalande C, Poggi G, Kennedy C, et al. Neuropsychological Outcome of Children Treated for Standard Risk Medulloblastoma in the PNET4 European Randomized Controlled Trial of Hyperfractionated Versus Standard Radiation Therapy and Maintenance Chemotherapy. Int J Radiat Oncol Biol Phys. 2015;92:978–985. doi: 10.1016/j.ijrobp.2015.04.023. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
