

Two-Year Outcomes of Surgical Treatment of Moderate Ischemic Mitral Regurgitation
- PMID: 27040451
- PMCID: PMC4908820
- DOI: 10.1056/NEJMoa1602003
Two-Year Outcomes of Surgical Treatment of Moderate Ischemic Mitral Regurgitation
Abstract
Background: In a trial comparing coronary-artery bypass grafting (CABG) alone with CABG plus mitral-valve repair in patients with moderate ischemic mitral regurgitation, we found no significant difference in the left ventricular end-systolic volume index (LVESVI) or survival after 1 year. Concomitant mitral-valve repair was associated with a reduced prevalence of moderate or severe mitral regurgitation, but patients had more adverse events. We now report 2-year outcomes.
Methods: We randomly assigned 301 patients to undergo either CABG alone or the combined procedure. Patients were followed for 2 years for clinical and echocardiographic outcomes.
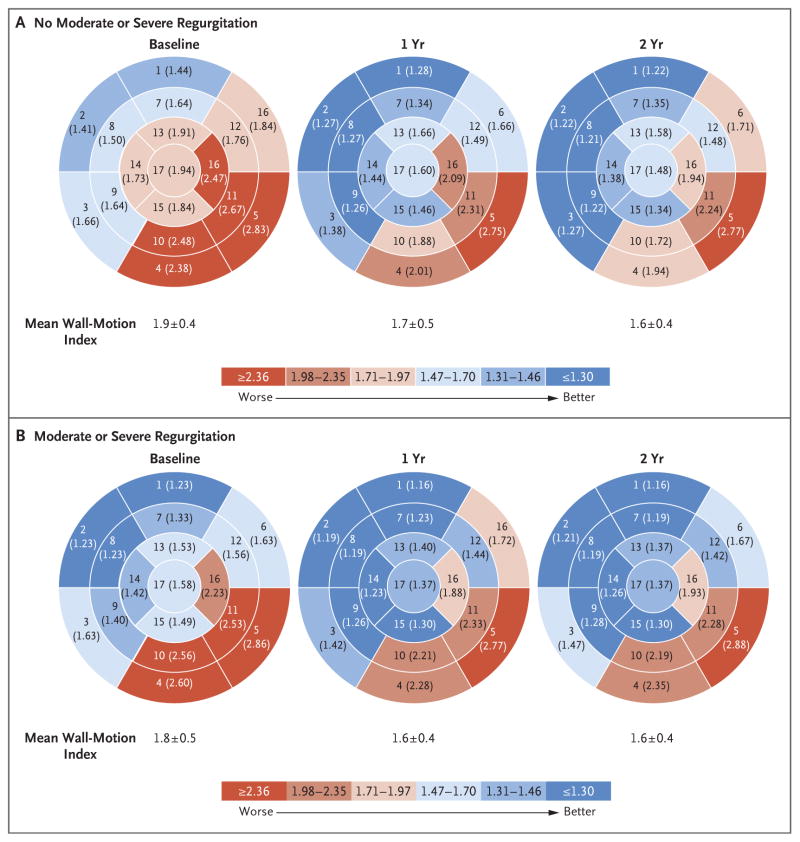
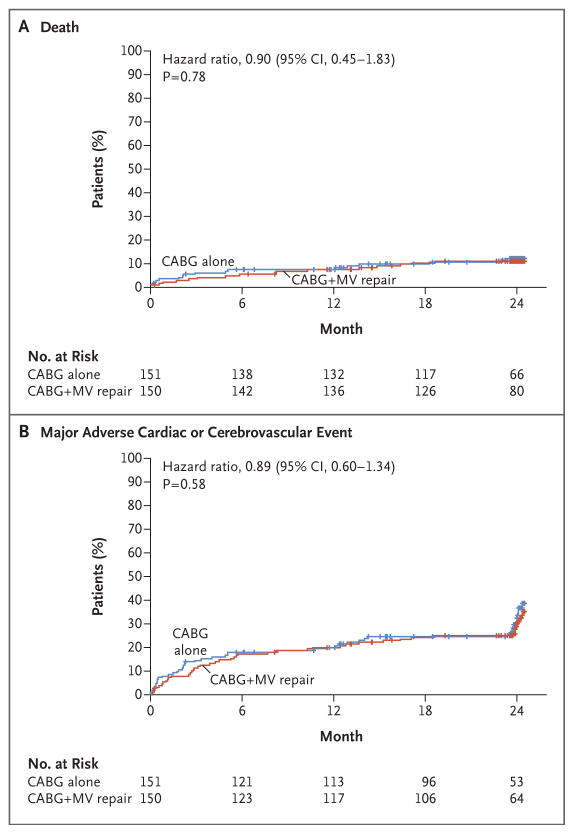
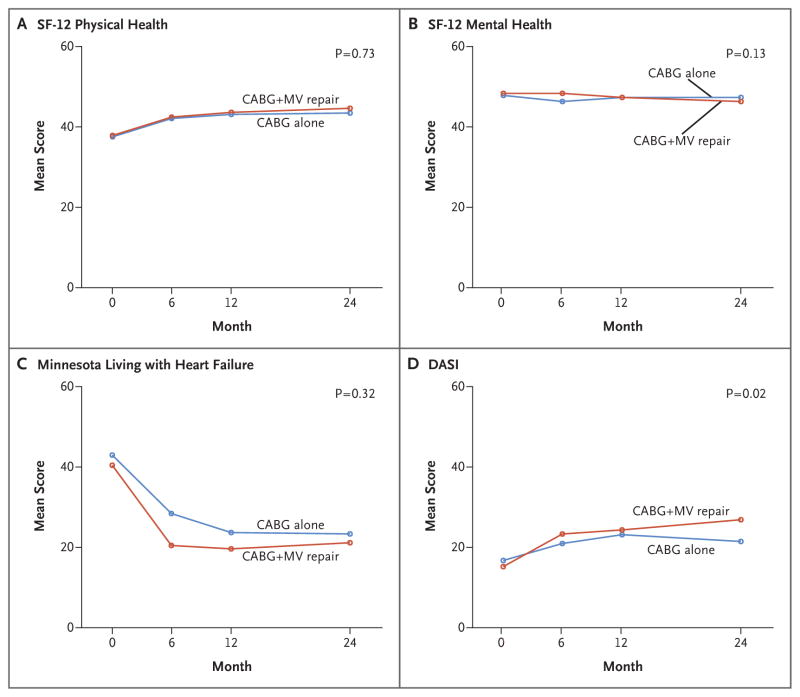
Results: At 2 years, the mean (±SD) LVESVI was 41.2±20.0 ml per square meter of body-surface area in the CABG-alone group and 43.2±20.6 ml per square meter in the combined-procedure group (mean improvement over baseline, -14.1 ml per square meter and -14.6 ml per square meter, respectively). The rate of death was 10.6% in the CABG-alone group and 10.0% in the combined-procedure group (hazard ratio in the combined-procedure group, 0.90; 95% confidence interval, 0.45 to 1.83; P=0.78). There was no significant between-group difference in the rank-based assessment of the LVESVI (including death) at 2 years (z score, 0.38; P=0.71). The 2-year rate of moderate or severe residual mitral regurgitation was higher in the CABG-alone group than in the combined-procedure group (32.3% vs. 11.2%, P<0.001). Overall rates of hospital readmission and serious adverse events were similar in the two groups, but neurologic events and supraventricular arrhythmias remained more frequent in the combined-procedure group.
Conclusions: In patients with moderate ischemic mitral regurgitation undergoing CABG, the addition of mitral-valve repair did not lead to significant differences in left ventricular reverse remodeling at 2 years. Mitral-valve repair provided a more durable correction of mitral regurgitation but did not significantly improve survival or reduce overall adverse events or readmissions and was associated with an early hazard of increased neurologic events and supraventricular arrhythmias. (Funded by the National Institutes of Health and Canadian Institutes of Health Research; ClinicalTrials.gov number, NCT00806988.).
Figures
Comment in
-
Mitral valve repair for moderate ischemic mitral regurgitation.J Thorac Dis. 2016 Jul;8(7):1410-3. doi: 10.21037/jtd.2016.05.41. J Thorac Dis. 2016. PMID: 27501403 Free PMC article. No abstract available.
-
Coronary artery bypass grafting (CABG) alone in moderate ischemic mitral regurgitation: is CABG really enough?Ann Transl Med. 2016 Oct;4(20):413. doi: 10.21037/atm.2016.08.47. Ann Transl Med. 2016. PMID: 27867965 Free PMC article. No abstract available.
-
Has moderate ischemic mitral regurgitation to be corrected?-Analysis of a randomized trial.Ann Transl Med. 2016 Oct;4(Suppl 1):S66. doi: 10.21037/atm.2016.10.57. Ann Transl Med. 2016. PMID: 27868034 Free PMC article. No abstract available.
References
-
- Bursi F, Enriquez-Sarano M, Nkomo VT, et al. Heart failure and death after myocardial infarction in the community: the emerging role of mitral regurgitation. Circulation. 2005;111:295–301. - PubMed
-
- Pérez de Isla L, Zamorano J, Quezada M, et al. Functional mitral regurgitation after a first non-ST-segment elevation acute coronary syndrome: contribution to congestive heart failure. Eur Heart J. 2007;28:2866–72. - PubMed
-
- Grigioni F, Detaint D, Avierinos JF, Scott C, Tajik J, Enriquez-Sarano M. Contribution of ischemic mitral regurgitation to congestive heart failure after myocardial infarction. J Am Coll Cardiol. 2005;45:260–7. - PubMed
-
- Penicka M, Linkova H, Lang O, et al. Predictors of improvement of unrepaired moderate ischemic mitral regurgitation in patients undergoing elective isolated coronary artery bypass graft surgery. Circulation. 2009;120:1474–81. - PubMed
-
- Roshanali F, Mandegar MH, Yousefnia MA, Alaeddini F, Wann S. Low-dose dobutamine stress echocardiography to predict reversibility of mitral regurgitation with CABG. Echocardiography. 2006;23:31–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical