

Personalized Immunomonitoring Uncovers Molecular Networks that Stratify Lupus Patients
- PMID: 27040498
- PMCID: PMC5426482
- DOI: 10.1016/j.cell.2016.03.008
Personalized Immunomonitoring Uncovers Molecular Networks that Stratify Lupus Patients
Erratum in
-
Personalized Immunomonitoring Uncovers Molecular Networks that Stratify Lupus Patients.Cell. 2016 Jun 2;165(6):1548-1550. doi: 10.1016/j.cell.2016.05.057. Cell. 2016. PMID: 27259156 No abstract available.
Abstract
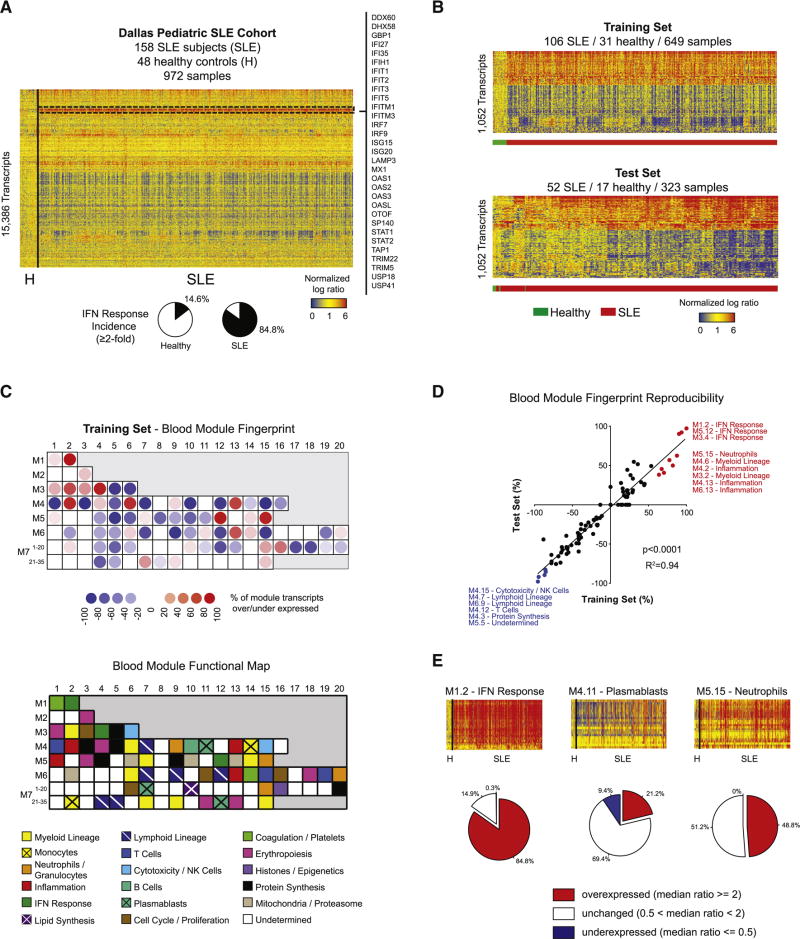
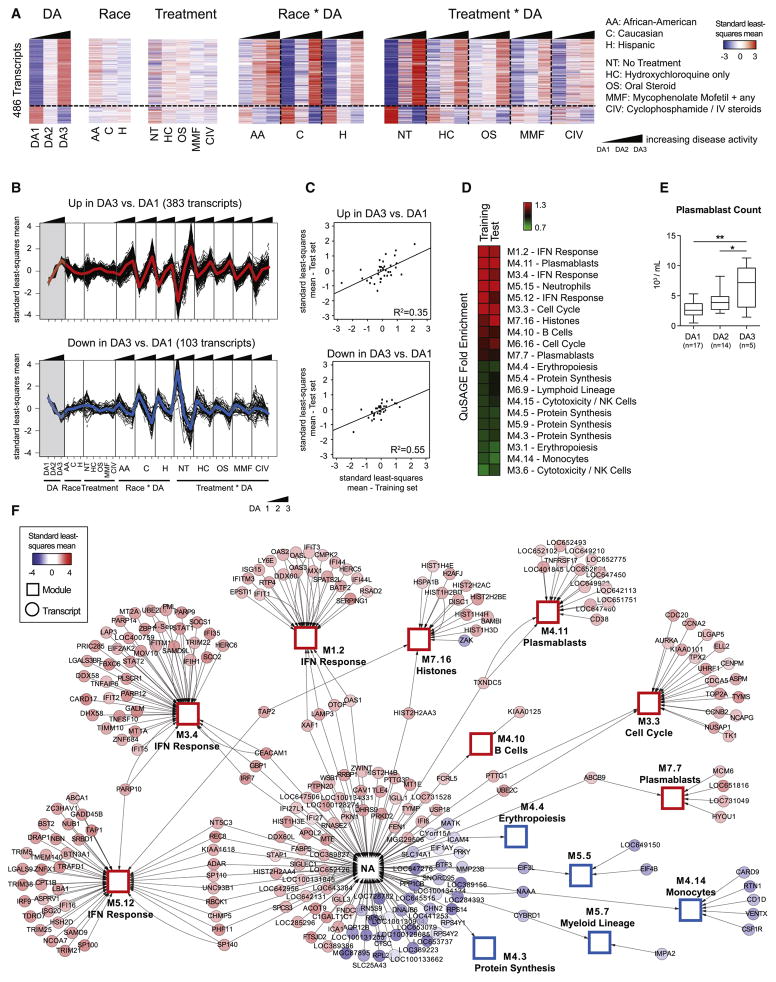
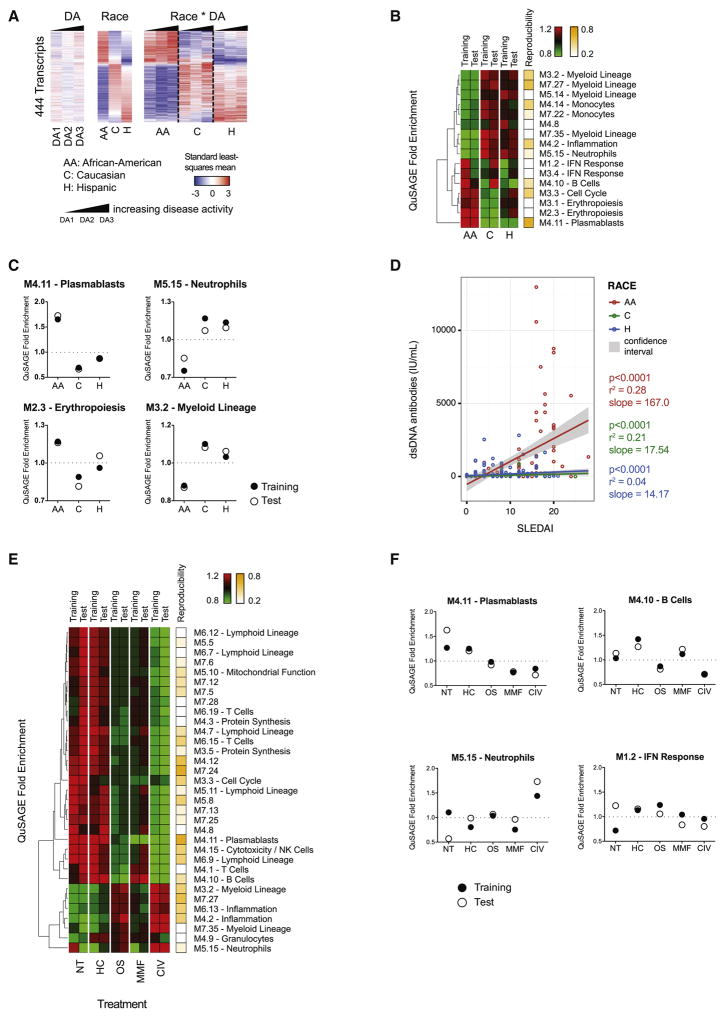
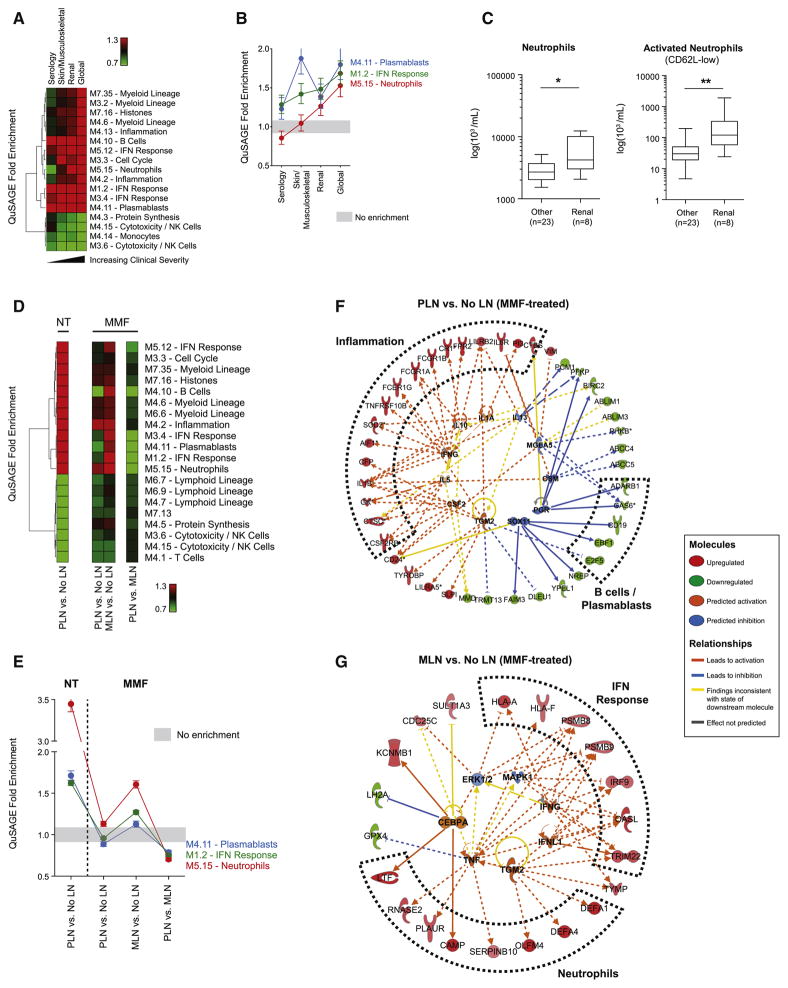
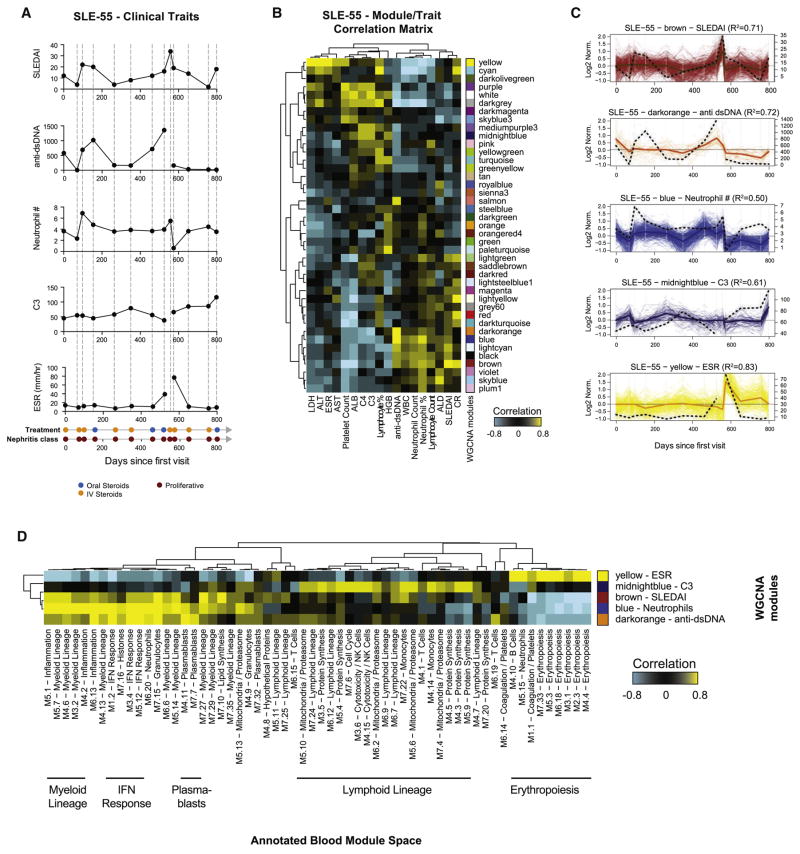
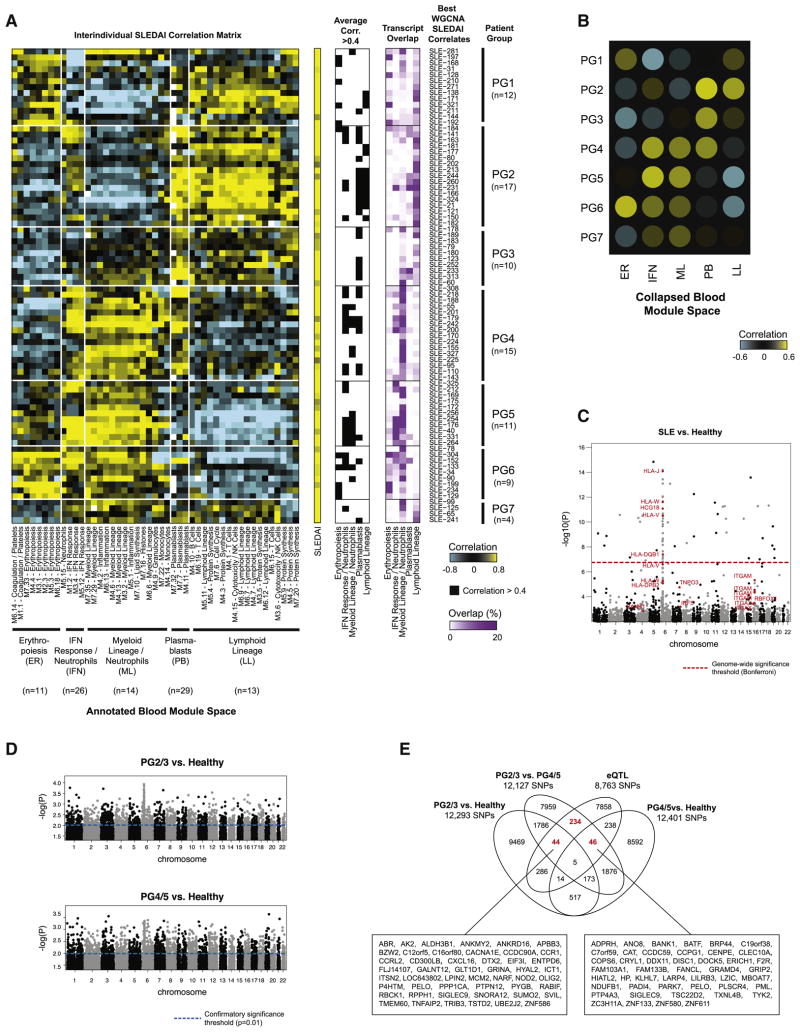
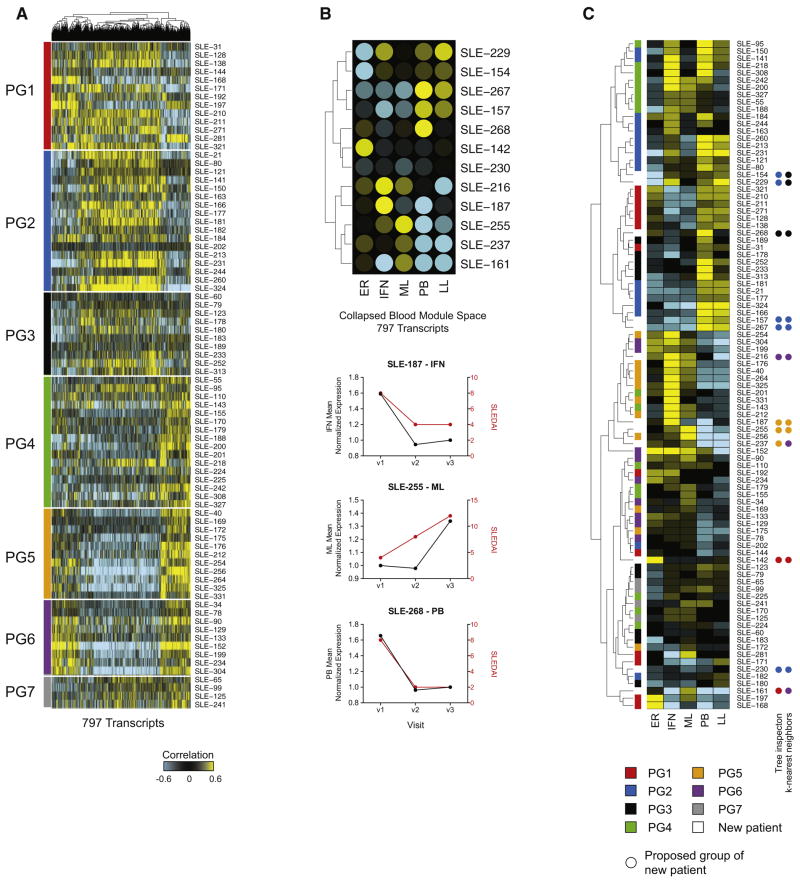
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by loss of tolerance to nucleic acids and highly diverse clinical manifestations. To assess its molecular heterogeneity, we longitudinally profiled the blood transcriptome of 158 pediatric patients. Using mixed models accounting for repeated measurements, demographics, treatment, disease activity (DA), and nephritis class, we confirmed a prevalent IFN signature and identified a plasmablast signature as the most robust biomarker of DA. We detected gradual enrichment of neutrophil transcripts during progression to active nephritis and distinct signatures in response to treatment in different nephritis subclasses. Importantly, personalized immunomonitoring uncovered individual correlates of disease activity that enabled patient stratification into seven groups, supported by patient genotypes. Our study uncovers the molecular heterogeneity of SLE and provides an explanation for the failure of clinical trials. This approach may improve trial design and implementation of tailored therapies in genetically and clinically complex autoimmune diseases. PAPERCLIP.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Glomerular disease: Personalized immunomonitoring in lupus and lupus nephritis.Nat Rev Nephrol. 2016 Jun;12(6):320-1. doi: 10.1038/nrneph.2016.69. Epub 2016 May 9. Nat Rev Nephrol. 2016. PMID: 27157443 No abstract available.
-
Introducing a New Dimension to Molecular Disease Classifications.Trends Mol Med. 2016 Jun;22(6):451-453. doi: 10.1016/j.molmed.2016.04.005. Epub 2016 May 5. Trends Mol Med. 2016. PMID: 27161597
References
-
- Arbuckle MR, McClain MT, Rubertone MV, Scofield RH, Dennis GJ, James JA, Harley JB. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. The New England journal of medicine. 2003;349:1526–1533. - PubMed
-
- Baechler EC, Batliwalla FM, Karypis G, Gaffney PM, Ortmann WA, Espe KJ, Shark KB, Grande WJ, Hughes KM, Kapur V, et al. Interferon-inducible gene expression signature in peripheral blood cells of patients with severe lupus. Proceedings of the National Academy of Sciences of the United States of America. 2003;100:2610–2615. - PMC - PubMed
-
- Bentham J, Morris DL, Cunninghame Graham DS, Pinder CL, Tombleson P, Behrens TW, Martin J, Fairfax BP, Knight JC, Chen L, et al. Genetic association analyses implicate aberrant regulation of innate and adaptive immunity genes in the pathogenesis of systemic lupus erythematosus. Nature genetics 2015 - PMC - PubMed
-
- Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, Urowitz M, Fortin PR, Petri M, Barr S, et al. Mortality in systemic lupus erythematosus. Arthritis and rheumatism. 2006;54:2550–2557. - PubMed
MeSH terms
Associated data
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
