

The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use
- PMID: 27041454
- PMCID: PMC5406132
- DOI: 10.1016/j.athoracsur.2015.12.074
The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use
Abstract
Background: Delirium is a common complication after cardiac surgical procedures and is associated with increased morbidity and mortality. However, whether rigorously assessed postoperative delirium is associated with an increased length of stay in the intensive care unit (LOS-ICU), length of stay (LOS), and hospital charges is not clear.
Methods: Patients (n = 66) undergoing coronary artery bypass or valve operations, or both, were enrolled in a nested cohort study. Rigorous delirium assessments were conducted using the Confusion Assessment Method. LOS-ICU and LOS were obtained from the medical record, and hospital charges were obtained from administrative data reported to the state. Because of the skewed distribution of outcome variables, outcomes were compared using rank-sum tests, as well as median regression incorporating propensity scores.
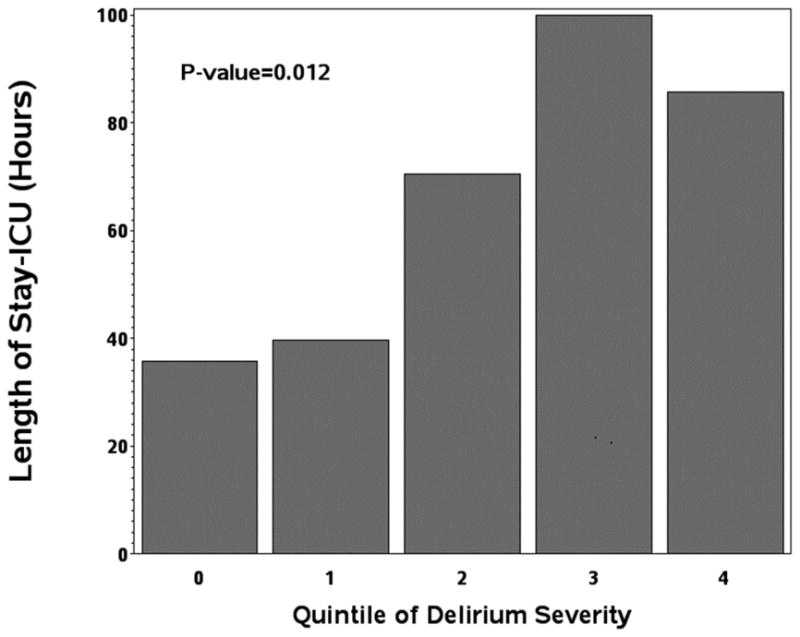
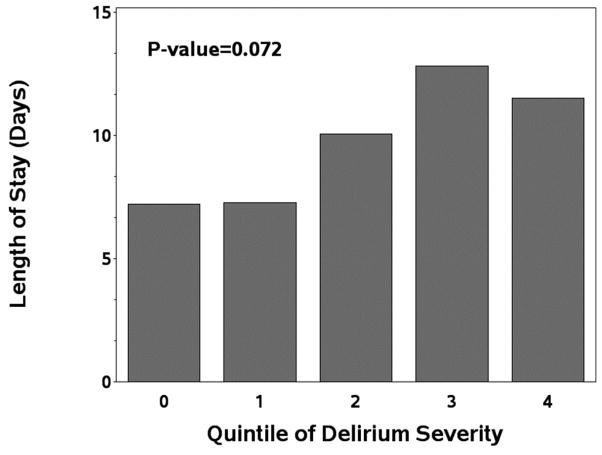
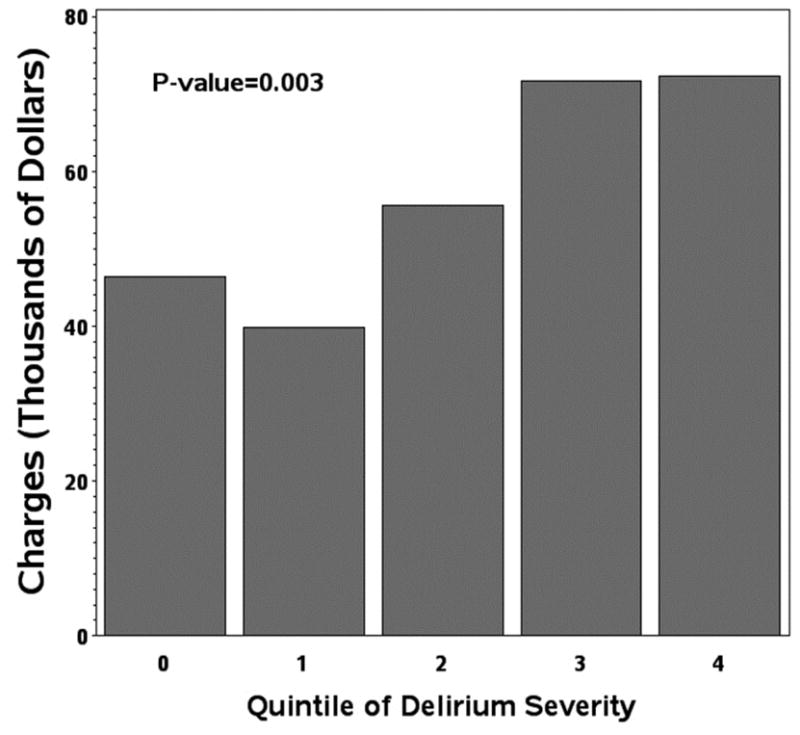
Results: Patients who developed delirium (56%) versus no delirium (43%) had increased median LOS-ICU (75.6 hours [interquartile range (IQR): 43.6 to 136.8] vs. 29.7 hours [IQR: 21.7 to 46.0]; p = 0.002), increased median LOS (9 days [IQR: 6 to 16] vs. 7 days [IQR: 5 to 8]; p = 0.006), and increased median hospital charges ($51,805 [IQR: $44,041 to $80,238] vs. $41,576 [IQR: $35,748 to $43,660]; p = 0.002). In propensity score models adjusted for patient-related and surgical characteristics and complications, the results for LOS-ICU and cost remained highly significant, although the results for LOS were attenuated on the basis of the specific statistical model. Increased severity of delirium was associated with both increased LOS-ICU and increased charges in a dose-response manner.
Conclusions: Delirium after cardiac surgical procedures is independently associated with both increased LOS-ICU and higher hospital charges. Because delirium is potentially preventable, targeted delirium-prevention protocols for high-risk patients may represent an important strategy for quality improvement.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Set conflict box: Dr Neufeld discloses a financial relationship with Ornim Medical; Dr Hogue with Ornim Medical and Covidien, Inc.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
