

Maxillary molar distalization with aligners in adult patients: a multicenter retrospective study
- PMID: 27041551
- PMCID: PMC4834290
- DOI: 10.1186/s40510-016-0126-0
Maxillary molar distalization with aligners in adult patients: a multicenter retrospective study
Abstract
Background: The aim of the present study was to test the hypothesis that bodily maxillary molar distalization was not achievable in aligner orthodontics.
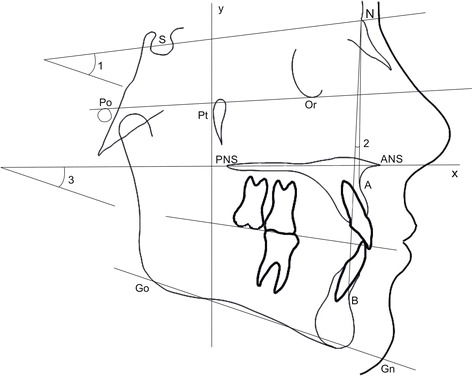
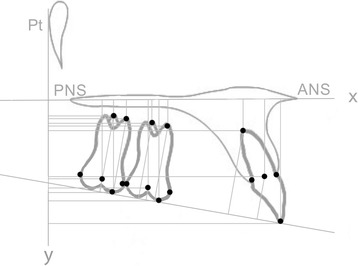
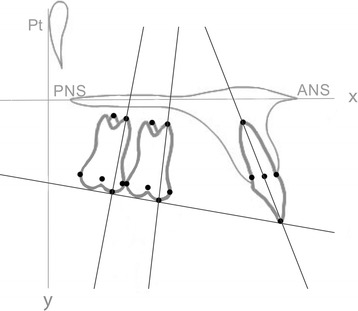
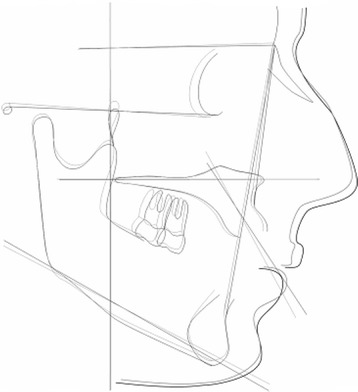
Methods: Forty lateral cephalograms obtained from 20 non-growing subjects (9 male, 11 female; average age 29.73 years) (group S), who underwent bilateral distalization of their maxillary dentition with Invisalign aligners (Align Technology, Inc., San José, CA, USA), were considered for the study. Skeletal class I or class II malocclusion and a bilateral end-to-end class II molar relationship were the main inclusion criteria. Cephalograms were taken at two time points: (T0) pretreatment and (T2) post-treatment. Treatment changes were evaluated between the time points using 39 variables by means of paired t test. The level of significance was set at P < 0.05. Reproducibility of measurements was assessed by the intraclass correlation coefficient (ICC).
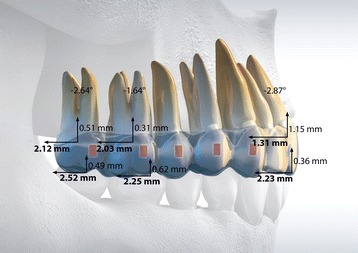
Results: The mean treatment time was 24.3 ± 4.2 months. At the post-treatment point, the first molar moved distally 2.25 mm without significant tipping (P = 0.27) and vertical movements (P = 0.43). The second molar distalization was 2.52 mm without significant tipping (P = 0.056) and vertical movements (P = 0.25). No significant movements were detected on the lower arch. SN^GoGn and SPP^GoGn angles showed no significant differences between pre- and post-treatment cephalograms (P = 0.22 and P = 0.85, respectively).
Conclusions: Aligner therapy in association with composite attachments and class II elastics can distalize maxillary first molars by 2.25 mm without significant tipping and vertical movements of the crown. No changes to the facial height were revealed.
Keywords: Adult patients; Aligners; Class II; Molar distalization.
Figures

References
-
- Bolla E, Muratore F, Carano A, Bowman SJ. Evaluation of maxillary molar distalization with the distal jet: a comparison with other contemporary methods. Angle Orthod. 2002;72:481–494. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
