

The outcomes of intra-aortic balloon pump usage in patients with acute myocardial infarction: a comprehensive meta-analysis of 33 clinical trials and 18,889 patients
- PMID: 27042021
- PMCID: PMC4801154
- DOI: 10.2147/PPA.S101945
The outcomes of intra-aortic balloon pump usage in patients with acute myocardial infarction: a comprehensive meta-analysis of 33 clinical trials and 18,889 patients
Abstract
Background: The effects of intra-aortic balloon pump (IABP) usage in patients with acute myocardial infarction remain controversial. This study sought to evaluate the outcomes of IABP usage in these patients.
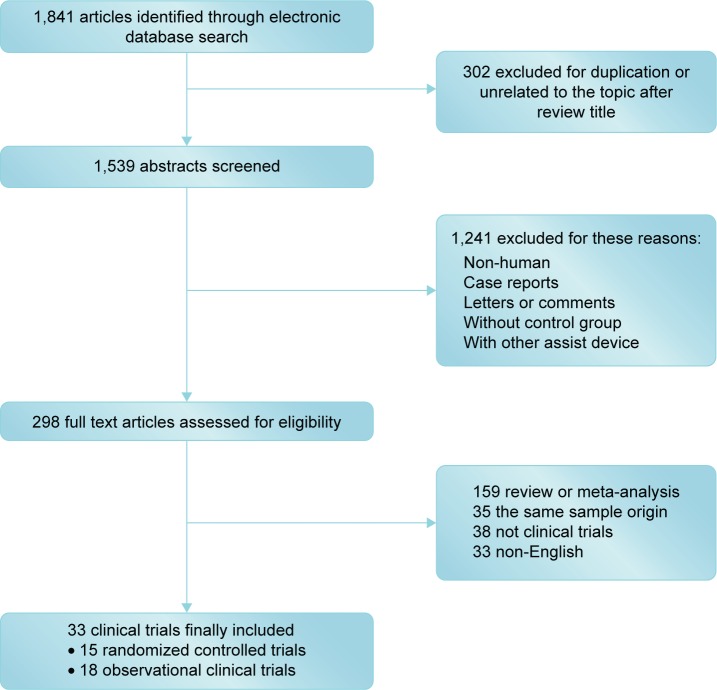
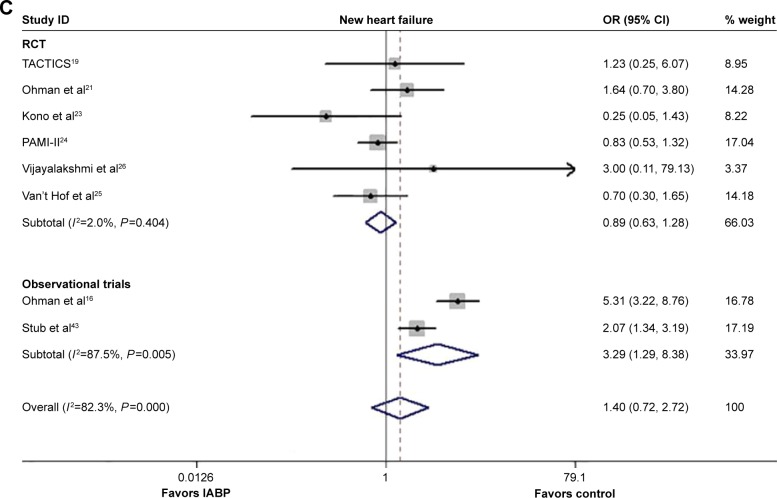
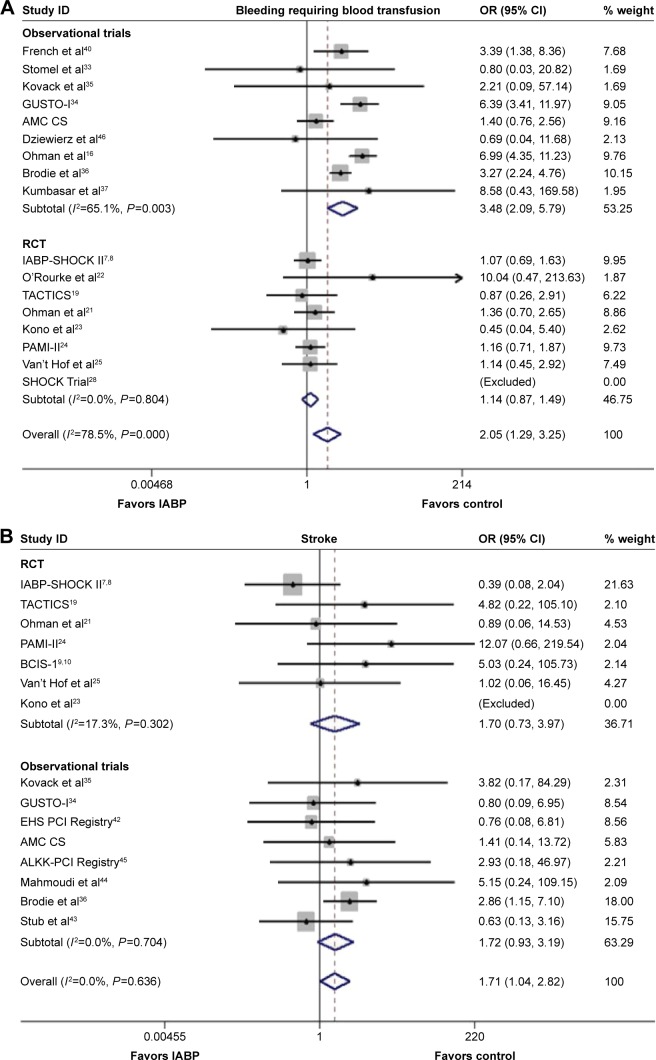
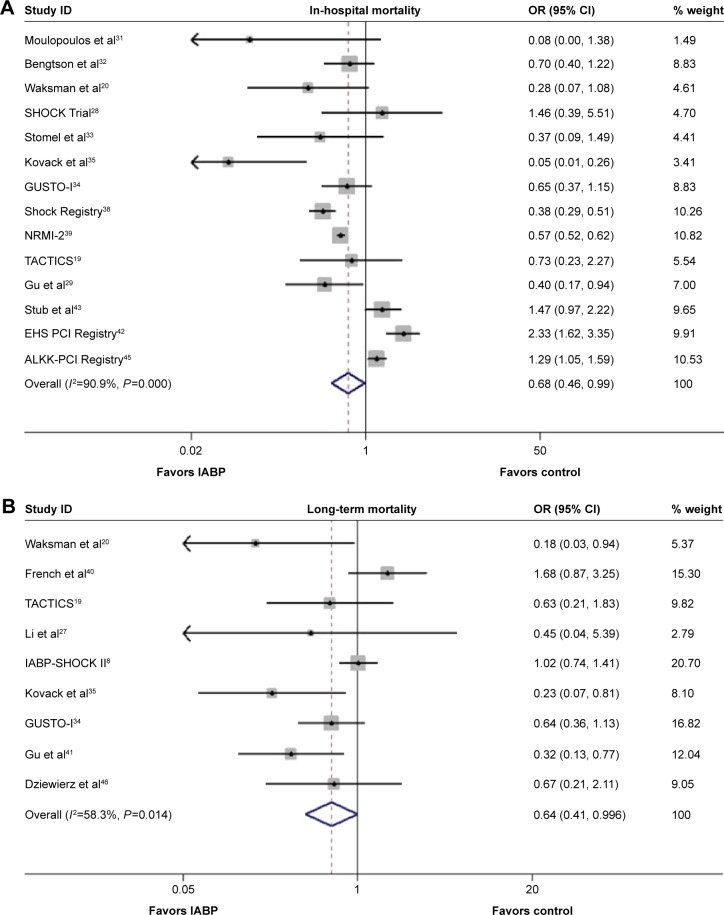
Methods: Medline, EMBASE, and other internet sources were searched for relevant clinical trials. The primary efficacy endpoints (in-hospital, midterm, and long-term mortality) and secondary endpoints (reinfarction, recurrent ischemia, and new heart failure in the hospital) as well as safety endpoints (severe bleeding requiring blood transfusion and stroke in-hospital) were subsequently analyzed.
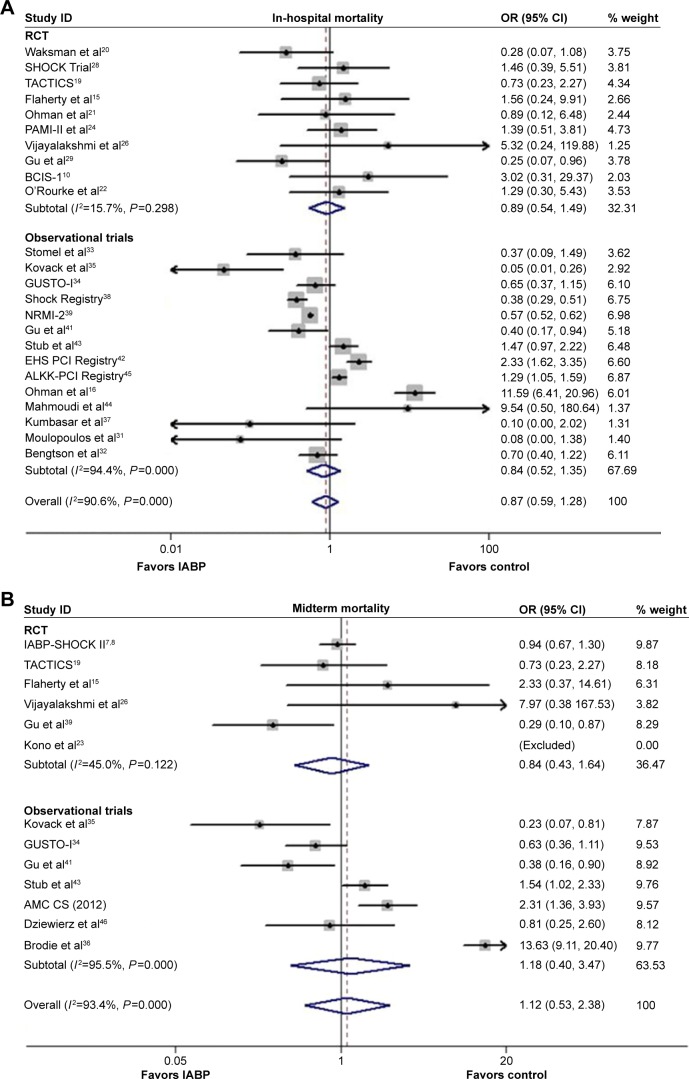
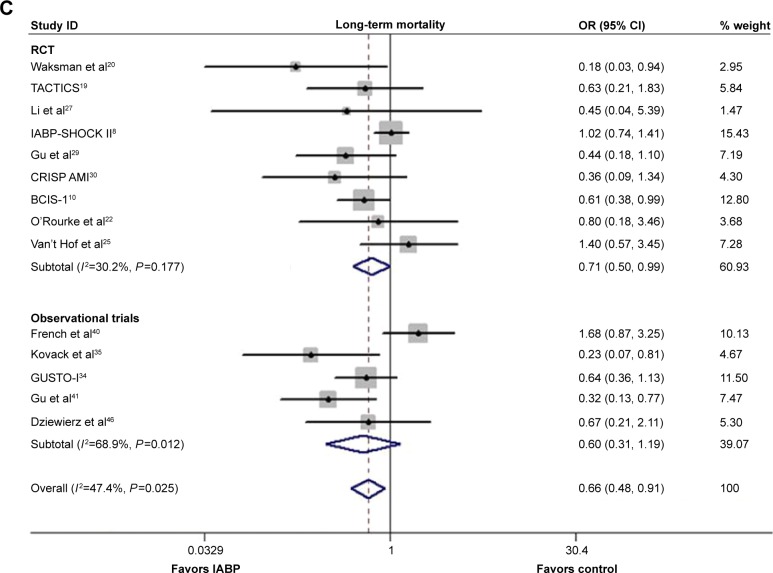
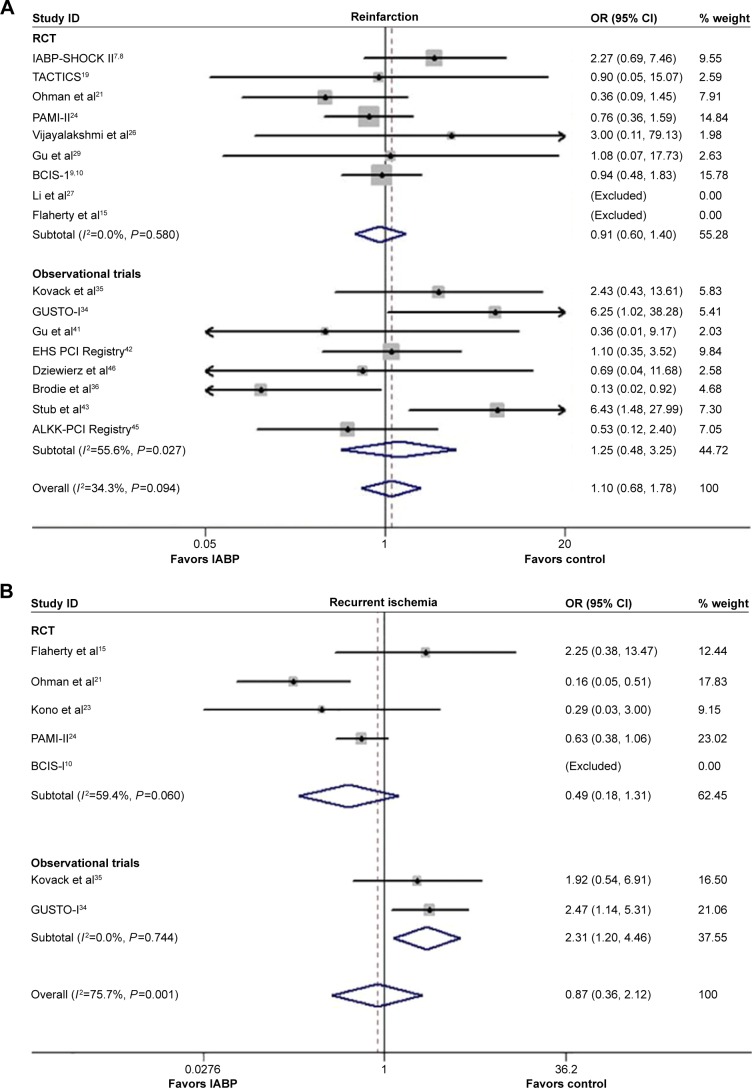
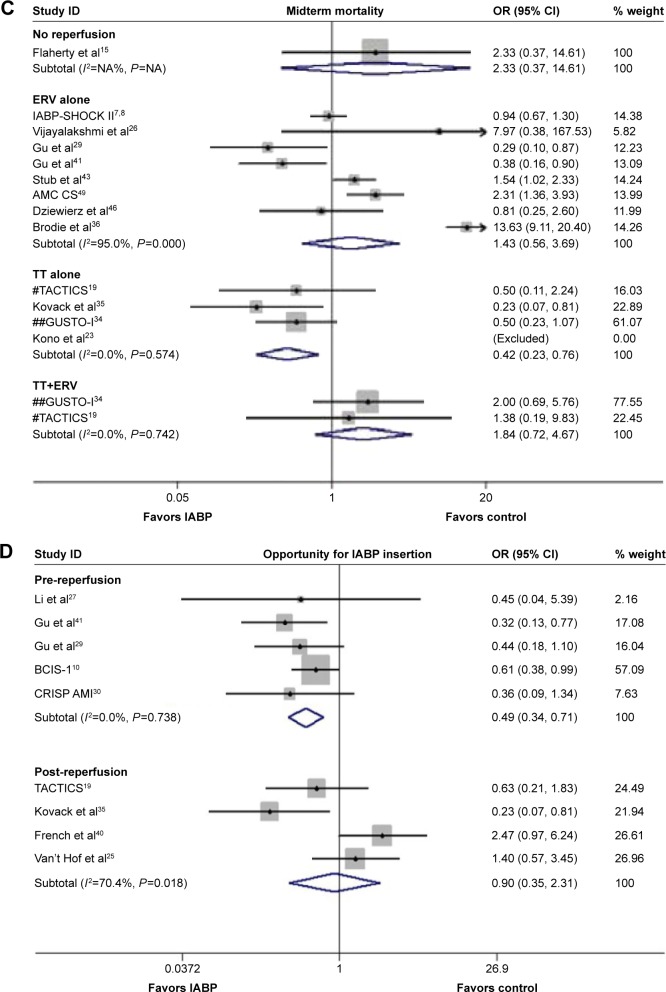
Results: Thirty-three clinical trials involving 18,889 patients were identified. The risk of long-term mortality in patients suffering from acute myocardial infarction was significantly decreased following IABP use (odds ratio [OR] 0.66, 95% confidence interval [CI]: 0.48-0.91, P=0.010). Both in-hospital and midterm mortality did not differ significantly between the IABP use group and no IABP use group (in-hospital: OR 0.87, 95% CI: 0.59-1.28, P=0.479; midterm: OR 1.12, 95% CI: 0.53-2.38, P=0.768). IABP insertion was not associated with the risk reduction of reinfarction, recurrent ischemia, or new heart failure. However, IABP use increased the risk of severe bleeding requiring blood transfusion (OR 2.05, 95% CI: 1.29-3.25, P=0.002) and stroke (OR 1.71, 95% CI: 1.04-2.82, P=0.035). In the thrombolytic therapy and cardiogenic shock subgroups, reduced mortality rates following IABP use were observed.
Conclusion: IABP insertion is associated with feasible benefits with respect to long-term survival rates in patients suffering from acute myocardial infarction, particularly those suffering from cardiogenic shock and receiving thrombolytic therapy, but at the cost of higher incidence of severe bleeding and stroke.
Keywords: acute myocardial infarction; cardiogenic shock; intra-aortic balloon pump; meta-analysis; thrombolytic therapy.
Figures
Similar articles
-
Impact of thrombolysis, intra-aortic balloon pump counterpulsation, and their combination in cardiogenic shock complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK?J Am Coll Cardiol. 2000 Sep;36(3 Suppl A):1123-9. doi: 10.1016/s0735-1097(00)00875-5. J Am Coll Cardiol. 2000. PMID: 10985715 Clinical Trial.
-
Predictors of mortality in patients with cardiogenic shock treated with primary percutaneous coronary intervention and intra-aortic balloon counterpulsation.Med Klin Intensivmed Notfmed. 2016 Nov;111(8):715-722. doi: 10.1007/s00063-015-0118-8. Epub 2015 Nov 23. Med Klin Intensivmed Notfmed. 2016. PMID: 26596273 English.
-
Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): final 12 month results of a randomised, open-label trial.Lancet. 2013 Nov 16;382(9905):1638-45. doi: 10.1016/S0140-6736(13)61783-3. Epub 2013 Sep 3. Lancet. 2013. PMID: 24011548 Clinical Trial.
-
Concomitant Intra-Aortic Balloon Pump Use in Cardiogenic Shock Requiring Veno-Arterial Extracorporeal Membrane Oxygenation.Circ Cardiovasc Interv. 2018 Sep;11(9):e006930. doi: 10.1161/CIRCINTERVENTIONS.118.006930. Circ Cardiovasc Interv. 2018. PMID: 30354593
-
The outcome of intra-aortic balloon pump support in acute myocardial infarction complicated by cardiogenic shock according to the type of revascularization: a comprehensive meta-analysis.Am Heart J. 2013 May;165(5):679-92. doi: 10.1016/j.ahj.2013.02.020. Epub 2013 Mar 26. Am Heart J. 2013. PMID: 23622904 Review.
Cited by
-
Stroke After Coronary Artery Bypass Grafting and Percutaneous Coronary Intervention: Incidence, Pathogenesis, and Outcomes.J Am Heart Assoc. 2019 Jul 2;8(13):e013032. doi: 10.1161/JAHA.119.013032. Epub 2019 Jun 27. J Am Heart Assoc. 2019. PMID: 31242821 Free PMC article. Review. No abstract available.
-
Incidence and Risk Factors for Stroke After Combined Heart-Kidney and Heart-Liver Transplantation.Clin Transplant. 2024 Jun;38(6):e15369. doi: 10.1111/ctr.15369. Clin Transplant. 2024. PMID: 39031709 Free PMC article.
-
Clinical and regulatory landscape for cardiogenic shock: A report from the Cardiac Safety Research Consortium ThinkTank on cardiogenic shock.Am Heart J. 2020 Jan;219:1-8. doi: 10.1016/j.ahj.2019.10.006. Epub 2019 Nov 7. Am Heart J. 2020. PMID: 31707323 Free PMC article. Review. No abstract available.
References
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119(9):1211–1219. - PMC - PubMed
-
- Scheidt S, Wilner G, Mueller H, et al. Intra-aortic balloon counter-pulsation in cardiogenic shock. Report of a co-operative clinical trial. N Engl J Med. 1973;288(19):979–984. - PubMed
-
- Kern MJ, Aguirre F, Bach R, Donohue T, Siegel R, Segal J. Augmentation of coronary blood flow by intra-aortic balloon pumping in patients after coronary angioplasty. Circulation. 1993;87(2):500–511. - PubMed
-
- Kantrowitz A, Tjonneland S, Freed PS, Phillips SJ, Butner AN, Sherman JL., Jr Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA. 1968;203(2):113–118. - PubMed
-
- Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction. J Am Coll Cardiol. 2013;61(23):e179–e347. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
