

Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: systematic review with meta-analysis
- PMID: 27042146
- PMCID: PMC4809334
- DOI: 10.2147/MDER.S103102
Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: systematic review with meta-analysis
Abstract
Background: Powered exoskeletons are designed to safely facilitate ambulation in patients with spinal cord injury (SCI). We conducted the first meta-analysis of the available published research on the clinical effectiveness and safety of powered exoskeletons in SCI patients.
Methods: MEDLINE and EMBASE databases were searched for studies of powered exoskeleton-assisted walking in patients with SCI. Main outcomes were analyzed using fixed and random effects meta-analysis models.
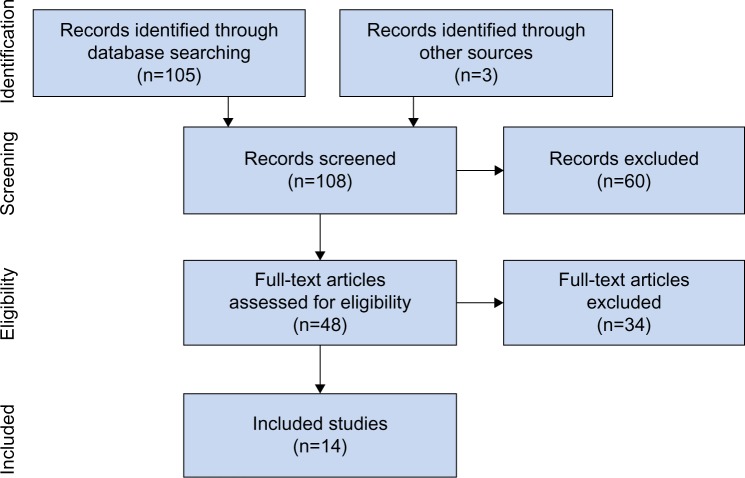
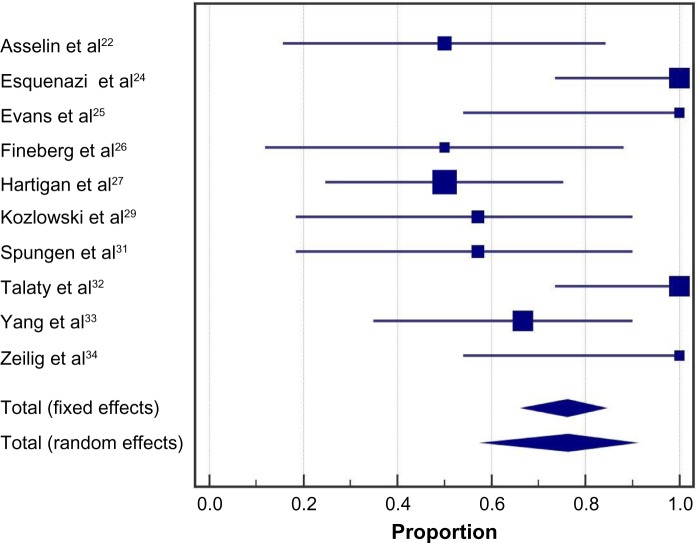
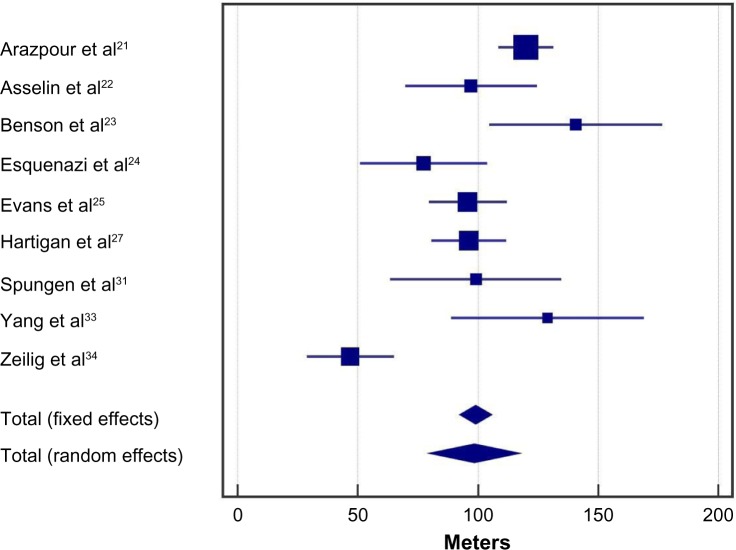
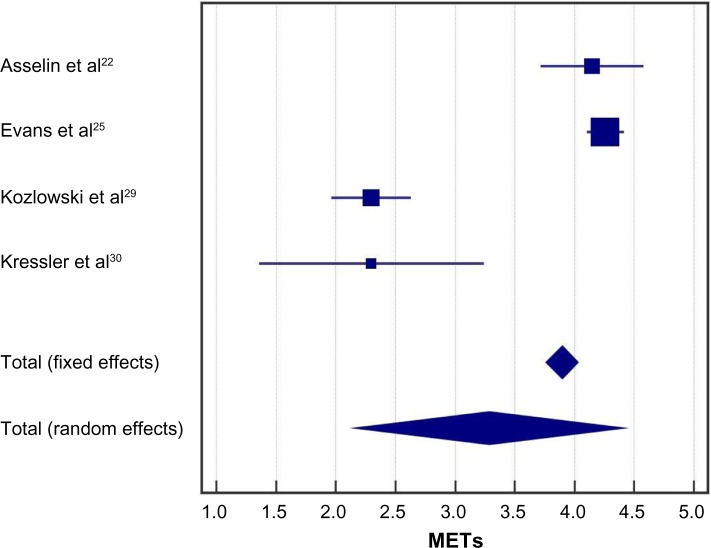
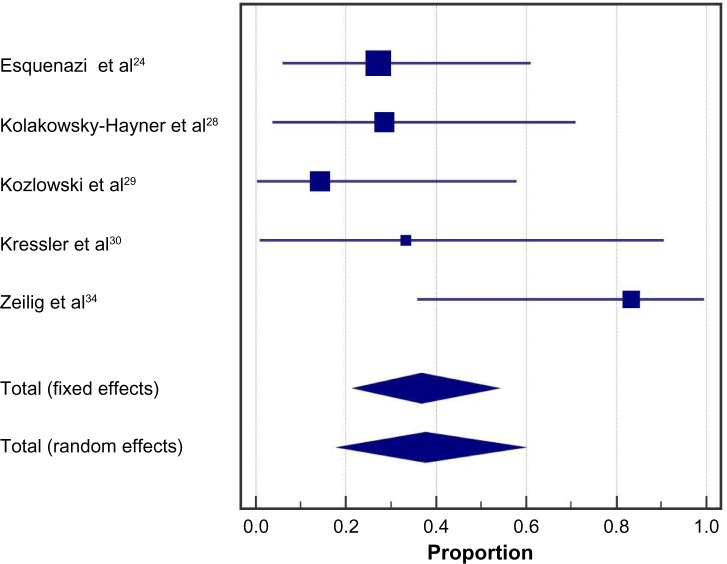
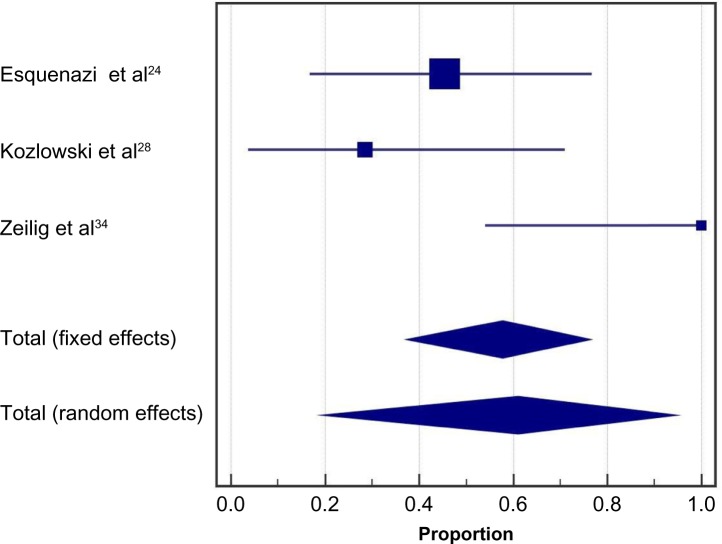
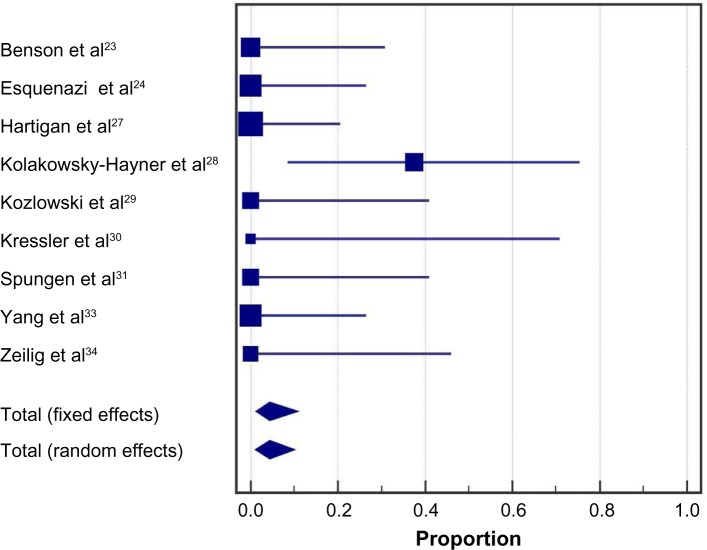
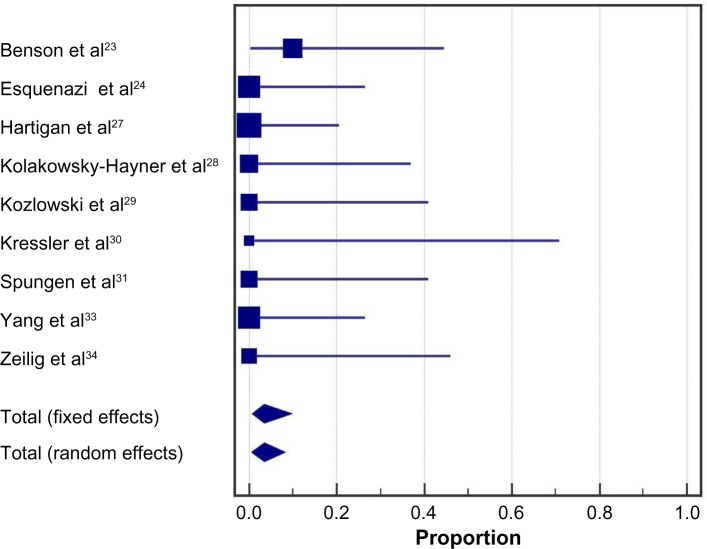
Results: A total of 14 studies (eight ReWalk™, three Ekso™, two Indego(®), and one unspecified exoskeleton) representing 111 patients were included in the analysis. Training programs were typically conducted three times per week, 60-120 minutes per session, for 1-24 weeks. Ten studies utilized flat indoor surfaces for training and four studies incorporated complex training, including walking outdoors, navigating obstacles, climbing and descending stairs, and performing activities of daily living. Following the exoskeleton training program, 76% of patients were able to ambulate with no physical assistance. The weighted mean distance for the 6-minute walk test was 98 m. The physiologic demand of powered exoskeleton-assisted walking was 3.3 metabolic equivalents and rating of perceived exertion was 10 on the Borg 6-20 scale, comparable to self-reported exertion of an able-bodied person walking at 3 miles per hour. Improvements in spasticity and bowel movement regularity were reported in 38% and 61% of patients, respectively. No serious adverse events occurred. The incidence of fall at any time during training was 4.4%, all occurring while tethered using a first-generation exoskeleton and none resulting in injury. The incidence of bone fracture during training was 3.4%. These risks have since been mitigated with newer generation exoskeletons and refinements to patient eligibility criteria.
Conclusion: Powered exoskeletons allow patients with SCI to safely ambulate in real-world settings at a physical activity intensity conducive to prolonged use and known to yield health benefits.
Keywords: Ekso; Indego; ReWalk; SCI; ambulation; orthosis.
Figures

Comment in
-
Letter to the editor regarding "Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: systematic review with meta-analysis".Med Devices (Auckl). 2016 Nov 29;9:419-421. doi: 10.2147/MDER.S125211. eCollection 2016. Med Devices (Auckl). 2016. PMID: 27942236 Free PMC article. No abstract available.
References
-
- Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal Cord. 2014;52(2):110–116. - PubMed
-
- Jensen MP, Truitt AR, Schomer KG, Yorks ton KM, Baylor C, Molton IR. Frequency and age effects of secondary health conditions in individuals with spinal cord injury: a scoping review. Spinal Cord. 2013;51(12):882–892. - PubMed
-
- Ditunno PL, Patrick M, Stineman M, Ditunno JF. Who wants to walk? Preferences for recovery after SCI: a longitudinal and cross-sectional study. Spinal Cord. 2008;46(7):500–506. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
