

Long-term healthcare use and costs in patients with stable coronary artery disease: a population-based cohort using linked health records (CALIBER)
- PMID: 27042338
- PMCID: PMC4816202
- DOI: 10.1093/ehjqcco/qcw003
Long-term healthcare use and costs in patients with stable coronary artery disease: a population-based cohort using linked health records (CALIBER)
Abstract
Aims: To examine long-term healthcare utilization and costs of patients with stable coronary artery disease (SCAD).
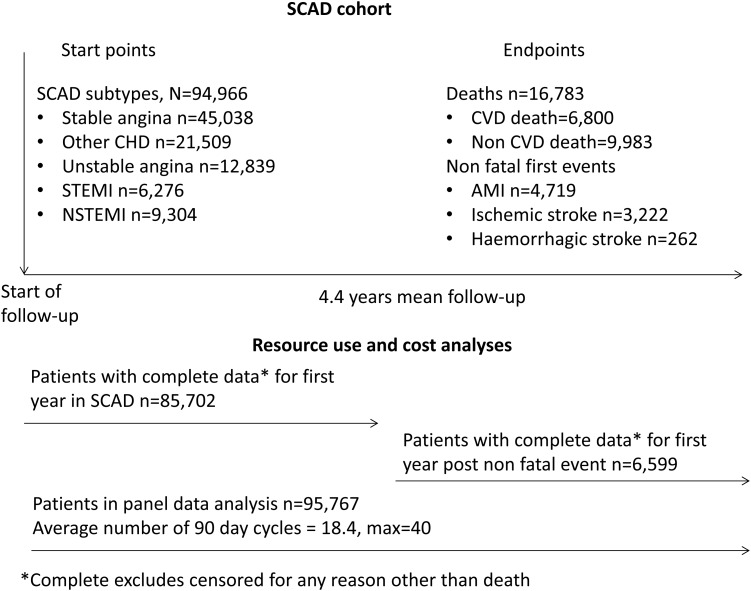
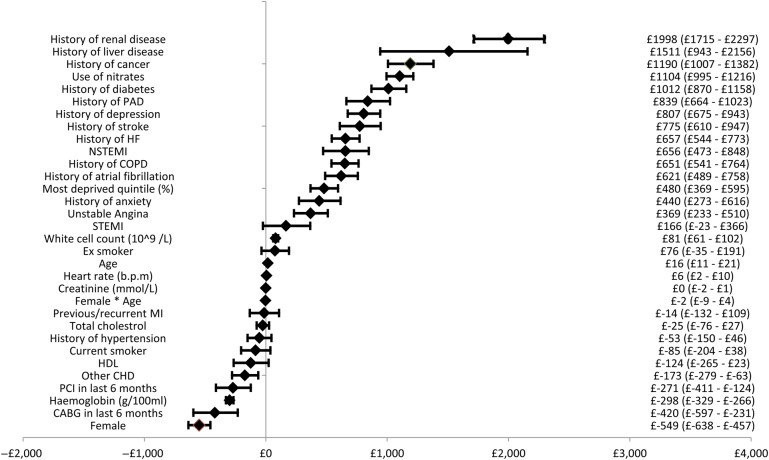
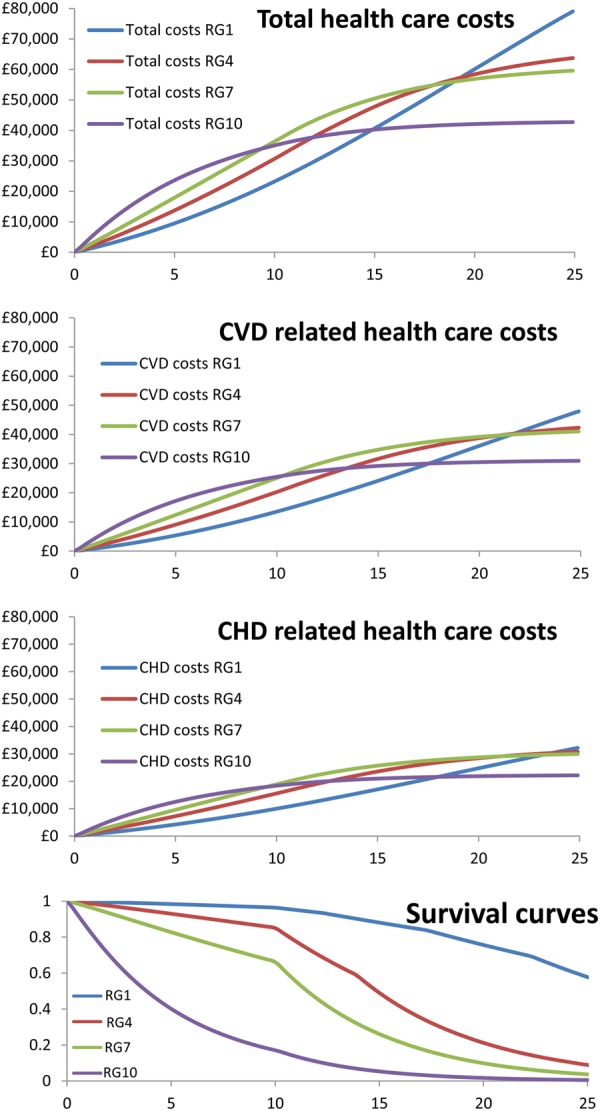
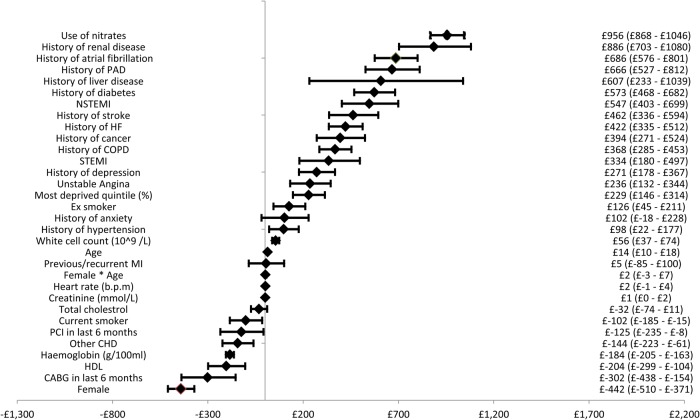
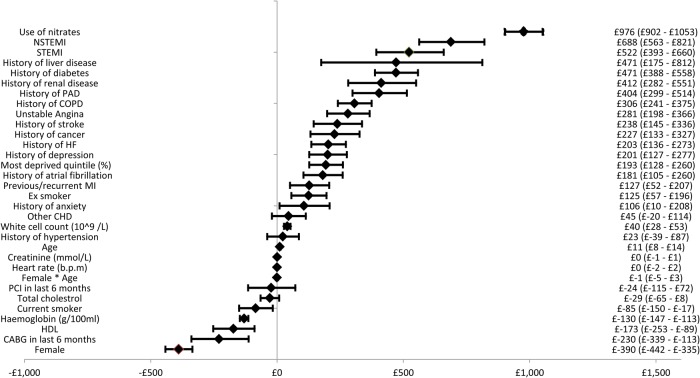
Methods and results: Linked cohort study of 94 966 patients with SCAD in England, 1 January 2001 to 31 March 2010, identified from primary care, secondary care, disease, and death registries. Resource use and costs, and cost predictors by time and 5-year cardiovascular disease (CVD) risk profile were estimated using generalized linear models. Coronary heart disease hospitalizations were 20.5% in the first year and 66% in the year following a non-fatal (myocardial infarction, ischaemic or haemorrhagic stroke) event. Mean healthcare costs were £3133 per patient in the first year and £10 377 in the year following a non-fatal event. First-year predictors of cost included sex (mean cost £549 lower in females), SCAD diagnosis (non-ST-elevation myocardial infarction cost £656 more than stable angina), and co-morbidities (heart failure cost £657 more per patient). Compared with lower risk patients (5-year CVD risk 3.5%), those of higher risk (5-year CVD risk 44.2%) had higher 5-year costs (£23 393 vs. £9335) and lower lifetime costs (£43 020 vs. £116 888).
Conclusion: Patients with SCAD incur substantial healthcare utilization and costs, which varies and may be predicted by 5-year CVD risk profile. Higher risk patients have higher initial but lower lifetime costs than lower risk patients as a result of shorter life expectancy. Improved cardiovascular survivorship among an ageing CVD population is likely to require stratified care in anticipation of the burgeoning demand.
Keywords: Costs; Electronic health records; Resource use; Stable coronary artery disease.
Figures
References
-
- Gale CP, Cattle BA, Woolston A, Baxter PD, West TH, Simms AD, Blaxill J, Greenwood DC, Fox KAA, West RM. Resolving inequalities in care? Reduced mortality in the elderly after acute coronary syndromes. The Myocardial Ischaemia National Audit Project 2003–2010. Eur Heart J 2012;33:630–639. - PubMed
-
- Gale CP, Allan V, Cattle BA, Hall AS, West RM, Timmis A, Gray HH, Deanfield J, Fox KAA, Feltbower R. Trends in hospital treatments, including revascularisation, following acute myocardial infarction, 2003–2010: a multilevel and relative survival analysis for the National Institute for Cardiovascular Outcomes Research (NICOR). Heart 2014;100:582–589. - PubMed
-
- Alabas OA, Allan V, McLenachan JM, Feltbower R, Gale CP. Age-dependent improvements in survival after hospitalisation with acute myocardial infarction: an analysis of the Myocardial Ischemia National Audit Project (MINAP). Age Ageing 2014;43:779–785. - PubMed
-
- Task Force Members, Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabaté M, Senior R, Taggart DP, van der Wall EE, Vrints CJ; ESC Committee for Practice Guidelines, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S; Document Reviewers, Knuuti J, Valgimigli M, Bueno H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gonzalez-Juanatey JR, Hamilos M, Hasdai D, Husted S, James SK, Kervinen K, Kolh P, Kristensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Rydén L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Windecker S, Yildirir A, Zamorano JL. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949–3003. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
