

CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios: better diagnostic markers of Alzheimer disease
- PMID: 27042676
- PMCID: PMC4774260
- DOI: 10.1002/acn3.274
CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios: better diagnostic markers of Alzheimer disease
Abstract
Objective: The diagnostic accuracy of cerebrospinal fluid (CSF) biomarkers for Alzheimer's disease (AD) must be improved before widespread clinical use. This study aimed to determine whether CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios are better diagnostic biomarkers of AD during both predementia and dementia stages in comparison to CSF Aβ42 alone.
Methods: The study comprised three different cohorts (n = 1182) in whom CSF levels of Aβ42, Aβ40, and Aβ38 were assessed. CSF Aβs were quantified using three different immunoassays (Euroimmun, Meso Scale Discovery, Quanterix). As reference standard, we used either amyloid ((18)F-flutemetamol) positron emission tomography (PET) imaging (n = 215) or clinical diagnosis (n = 967) of well-characterized patients.
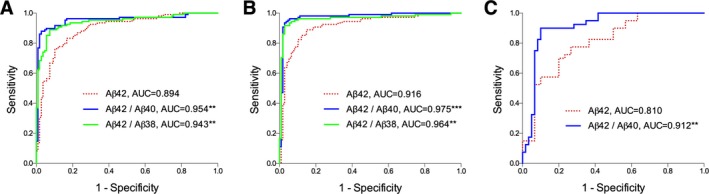
Results: When using three different immunoassays in cases with subjective cognitive decline and mild cognitive impairment, the CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios were significantly better predictors of abnormal amyloid PET than CSF Aβ42. Lower Aβ42, Aβ42/Aβ40, and Aβ42/Aβ38 ratios, but not Aβ40 and Aβ38, correlated with smaller hippocampal volumes measured by magnetic resonance imaging. However, lower Aβ38, Aβ40, and Aβ42, but not the ratios, correlated with non-AD-specific subcortical changes, that is, larger lateral ventricles and white matter lesions. Further, the Aβ42/Aβ40 and Aβ42/Aβ38 ratios showed increased accuracy compared to Aβ42 when distinguishing AD from dementia with Lewy bodies or Parkinson's disease dementia and subcortical vascular dementia, where all Aβs (including Aβ42) were decreased.
Interpretation: The CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios are significantly better than CSF Aβ42 to detect brain amyloid deposition in prodromal AD and to differentiate AD dementia from non-AD dementias. The ratios reflect AD-type pathology better, whereas decline in CSF Aβ42 is also associated with non-AD subcortical pathologies. These findings strongly suggest that the ratios rather than CSF Aβ42 should be used in the clinical work-up of AD.
Figures



References
-
- Wilquet V, De Strooper B. Amyloid‐beta precursor protein processing in neurodegeneration. Curr Opin Neurobiol 2004;14:582–588. - PubMed
-
- Portelius E, Price E, Brinkmalm G, et al. A novel pathway for amyloid precursor protein processing. Neurobiol Aging 2011;32:1090–1098. - PubMed
-
- Sanchez L, Madurga S, Pukala T, et al. Abeta40 and Abeta42 amyloid fibrils exhibit distinct molecular recycling properties. J Am Chem Soc 2011;133:6505–6508. - PubMed
-
- Iwatsubo T, Odaka A, Suzuki N, et al. Visualization of A beta 42(43) and A beta 40 in senile plaques with end‐specific A beta monoclonals: evidence that an initially deposited species is A beta 42(43). Neuron 1994;13:45–53. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
