

Mild Cognitive Impairment
- PMID: 27042901
- PMCID: PMC5390929
- DOI: 10.1212/CON.0000000000000313
Mild Cognitive Impairment
Abstract
Purpose of review: As individuals age, the quality of cognitive function becomes an increasingly important topic. The concept of mild cognitive impairment (MCI) has evolved over the past 2 decades to represent a state of cognitive function between that seen in normal aging and dementia. As such, it is important for health care providers to be aware of the condition and place it in the appropriate clinical context.
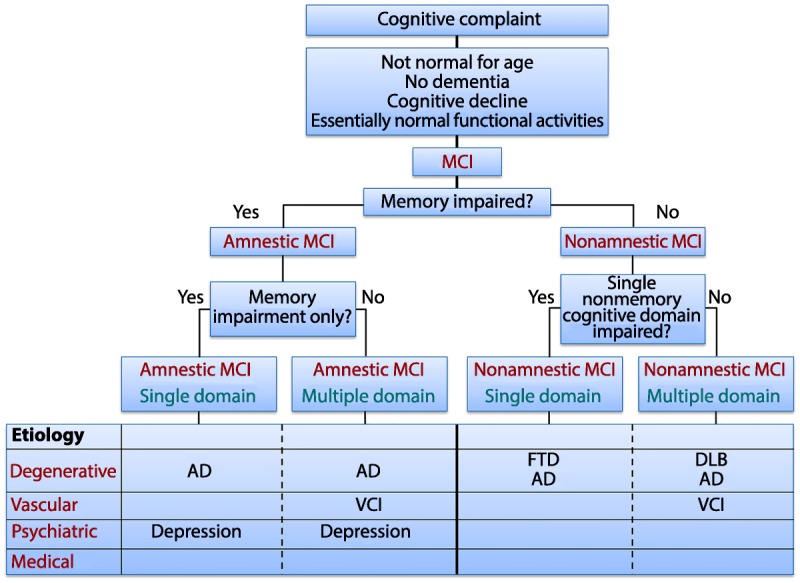
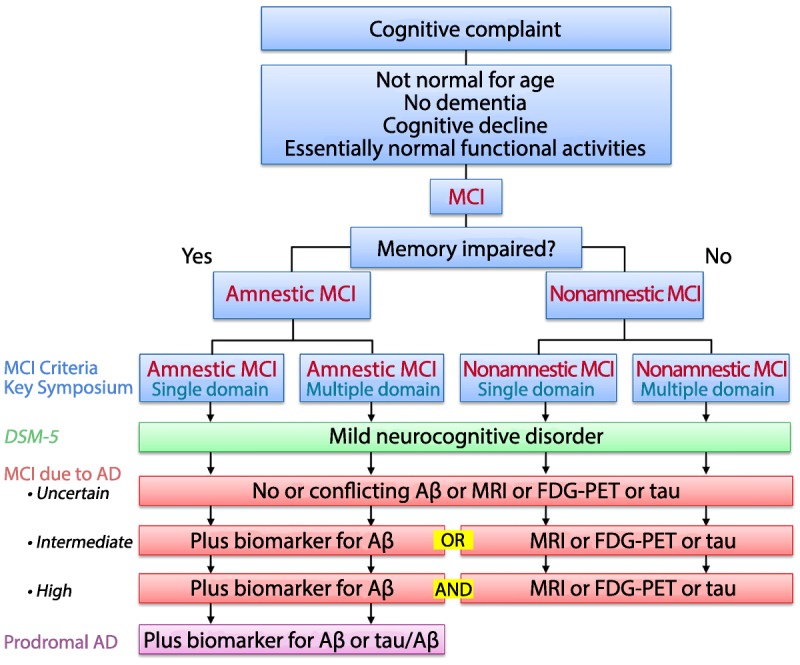
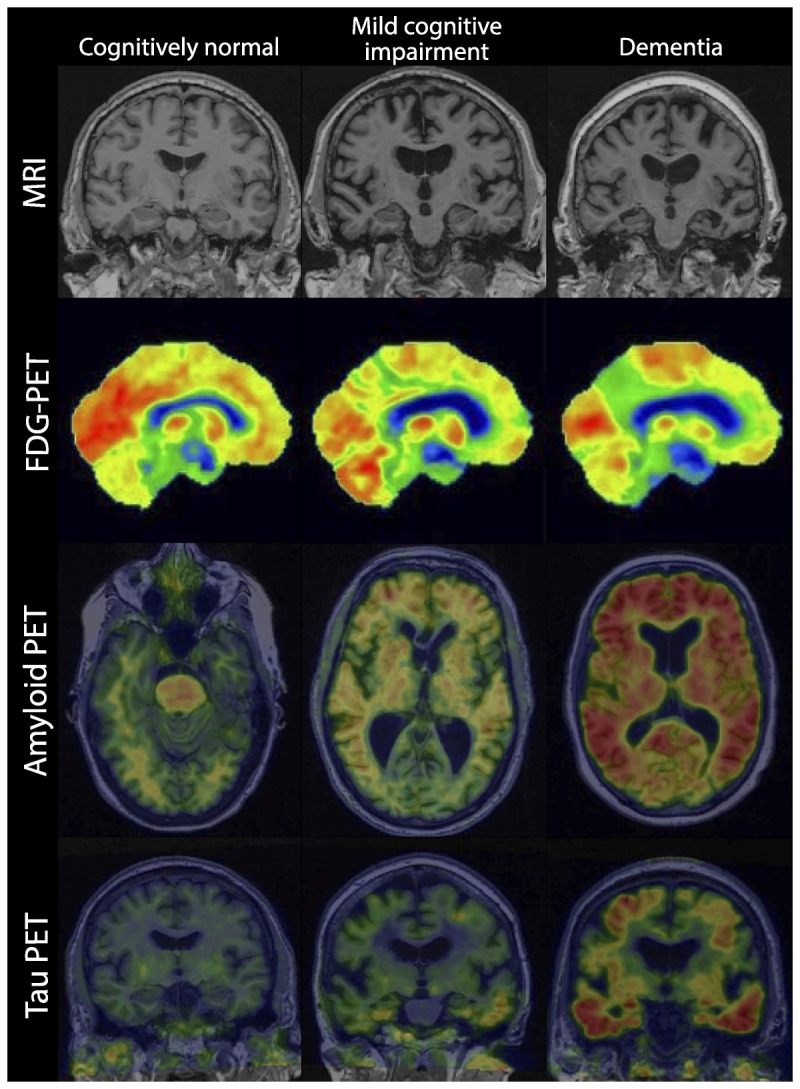
Recent findings: Numerous international population-based studies have been conducted to document the frequency of MCI, estimating its prevalence to be between 15% and 20% in persons 60 years and older, making it a common condition encountered by clinicians. The annual rate in which MCI progresses to dementia varies between 8% and 15% per year, implying that it is an important condition to identify and treat. In those MCI cases destined to develop Alzheimer disease, biomarkers are emerging to help identify etiology and predict progression. However, not all MCI is due to Alzheimer disease, and identifying subtypes is important for possible treatment and counseling. If treatable causes are identified, the person with MCI might improve.
Summary: MCI is an important clinical entity to identify, and while uncertainties persist, clinicians need to be aware of its diagnostic features to enable them to counsel patients. MCI remains an active area of research as numerous randomized controlled trials are being conducted to develop effective treatments.
Figures
References
-
- Jack CR, Jr, Albert MS, Knopman DS, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & dementia: the journal of the Alzheimer’s Association 2011; 7(3): 257– 262. doi:10.1016/j.jalz.2011.03.004. - PMC - PubMed
-
- Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med 2004; 256(3): 183– 194. doi:10.1111/j.1365-2796.2004.01388.x. - PubMed
-
- Petersen RC. Clinical practice. Mild cognitive impairment. N Engl J Med 2011; 364(23): 2227– 2234. doi:10.1056/NEJMcp0910237. - PubMed
-
- Reisberg B, Ferris S, de Leon MJ. Stage-specific behavioral, cognitive, and in vivo changes in community residing subjects with age-associated memory impairment and primary degenerative dementia of the Alzheimer type. Drug Dev Res 1988; 15(2–3): 101– 114. doi:10.1002/ddr.430150203.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous