

Rationale and design of the European Polyp Surveillance (EPoS) trials
- PMID: 27042931
- PMCID: PMC5412707
- DOI: 10.1055/s-0042-104116
Rationale and design of the European Polyp Surveillance (EPoS) trials
Abstract
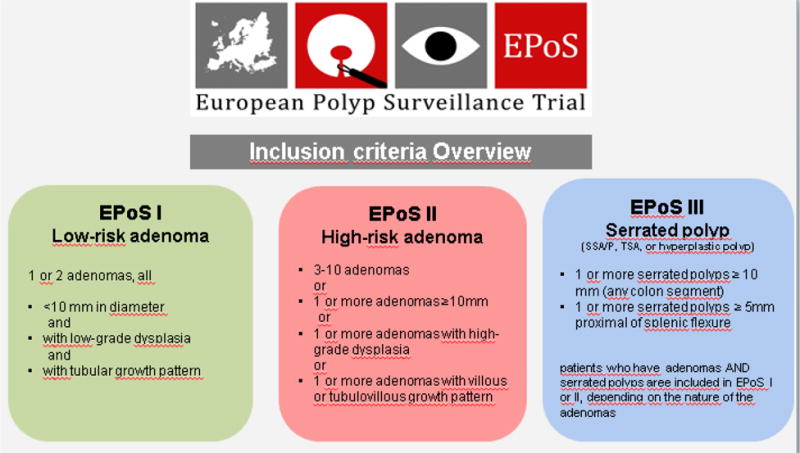
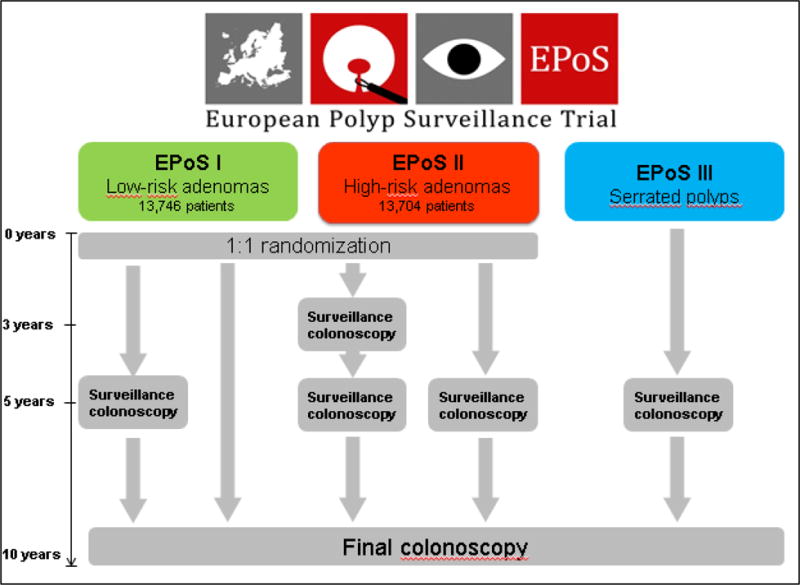
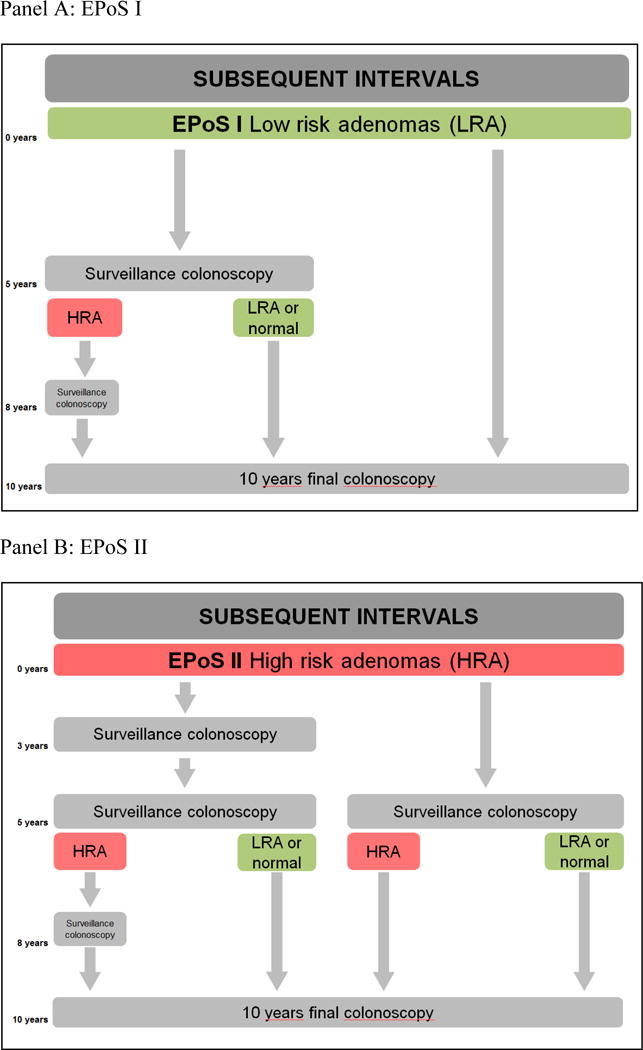
Background: Current guidelines recommend surveillance colonoscopies after polyp removal depending on the number and characteristics of polyps, but there is a lack of evidence supporting the recommendations. This report outlines the rationale and design of two randomized trials and one observational study investigating evidence-based surveillance strategies following polyp removal. Study design and endpoints: The EPoS studies started to recruit patients in April 2015. EPoS study I randomizes 13 746 patients with low-risk adenomas (1 - 2 tubular adenomas size < 10 mm, low-grade dysplasia) to surveillance after 5 and 10 years, or 10 years only. EPoS study II randomizes 13 704 patients with high-risk adenomas (3 - 10 adenomas or adenoma ≥ 10 mm in diameter, or adenoma with high-grade dysplasia, or > 25 % villous features) to surveillance after 3, 5, and 10 years, or 5 and 10 years only. EPoS study III offers surveillance after 5 and 10 years to patients with serrated polyps ≥ 10 mm in diameter at any location, or serrated polyps ≥ 5 mm in diameter proximal to the splenic flexure. All polyps are removed before patients enter the trials. The primary end point is colorectal cancer incidence after 10 years. We assume a colorectal cancer risk of 1 % for patients in EPoS I, and 2 % for patients in EPoS II. Using a noninferiority hypothesis with an equivalence interval of 0.5 % for EPoS I and 0.7 % for EPoS II, the trials are 90 % powered to uncover differences larger than the equivalence intervals. For EPoS III, no power analyses have been performed.
Conclusions: The present trials aim to develop evidence-based strategies for polyp surveillance, thereby maximizing effectiveness and minimizing resources.
Trial registration: ClinicalTrials.gov (NCT02319928).
© Georg Thieme Verlag KG Stuttgart · New York.
Figures
Comment in
-
French comment on article: Rational and design of the European Polyp Surveillance (EPoS) trials.Endoscopy. 2016 Jun;48(6):604. doi: 10.1055/s-0042-108249. Epub 2016 May 30. Endoscopy. 2016. PMID: 27239834 No abstract available.
References
-
- GLOBOCAN Database. International Agency for Research on Cancer. World Health Organization; 2008. http://globocan.iarc.fr/
-
- Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–32. - PubMed
-
- Ijspeert JE, Vermeulen L, Meijer GA, Dekker E. Serrated neoplasia-role in colorectal carcinogenesis and clinical implications. Nat Rev Gastroenterol Hepatol. 2015;12:401–9. - PubMed
-
- Bretthauer M. Evidence for colorectal cancer screening. Best Practice & Research Clinical Gastroenterology. 2010;24:417–425. - PubMed
-
- Bretthauer M, Kalager M. Colonoscopy as a triage screening test. N Engl J Med. 2012;366:759–60. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
