

Case Reports
doi: 10.7326/M15-3066.
Epub 2016 Apr 5.
Severe Meningoencephalitis in a Case of Ebola Virus Disease: A Case Report
- PMID: 27043004
- PMCID: PMC5089366
- DOI: 10.7326/M15-3066
Item in Clipboard
Case Reports
Severe Meningoencephalitis in a Case of Ebola Virus Disease: A Case Report
Ann Intern Med.
.
No abstract available
Figures
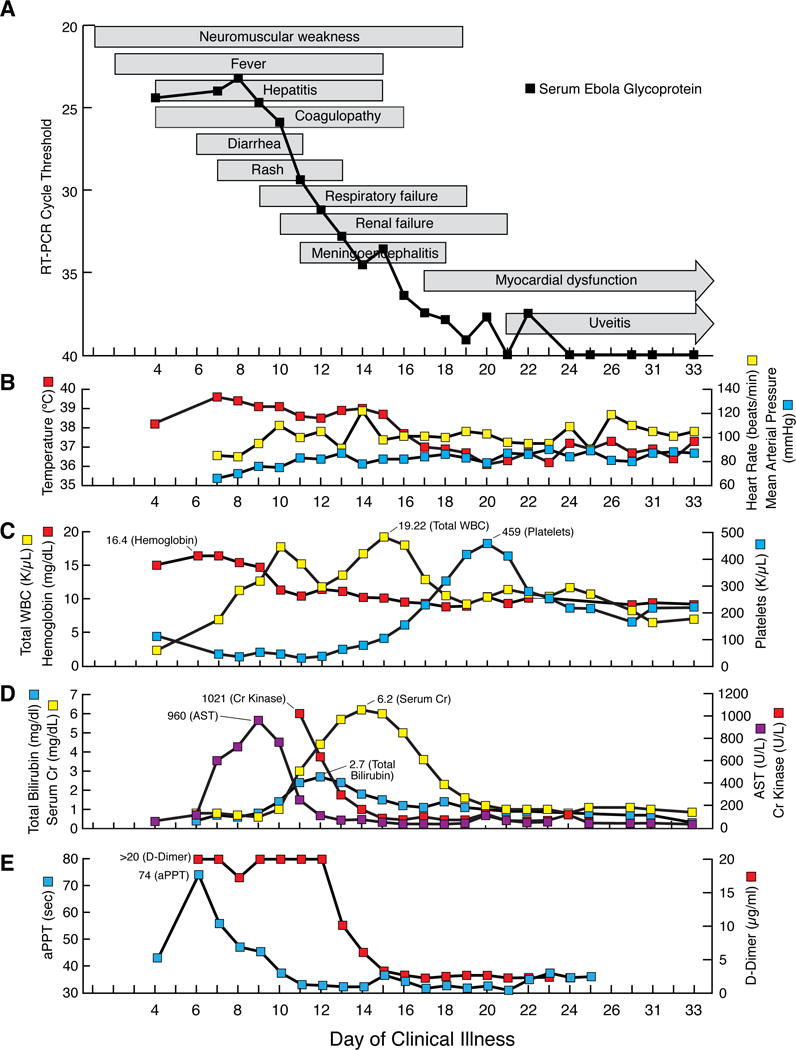
Sequential multi-organ failure in a patient with Ebola virus disease despite adequate blood pressure control: (A–E) Clinical course (A) text-boxes show approximate onset and resolution of clinical findings. Line-graph shows cycle threshold value that Ebola virus glycoprotein RNA was detected by quantitative reverse transcriptase polymerase chain reaction (RT-PCR) in serum. Select vital signs (B) red line-graph shows maximum daily temperature, yellow line-graph shows maximum daily heart rate, and blue line-graph shows minimum daily mean arterial blood pressure. Select laboratory values (C–E). Complete blood count (C) red line-graph show hemoglobin level, yellow line-graph shows total white blood cell (WBC) count, and blue line-graph shows platelet count. Serum chemistries (D) purple line-graph shows aspartate aminotransferase (AST) level, blue line-graph shows total bilirubin level, red line-graph shows creatinine kinase level, and yellow line-graph shows serum creatinine (Cr) level. Coagulation (E) blue line-graph shows activated partial thromboplastin (aPPT) level and red line-graph shows d-dimer level.
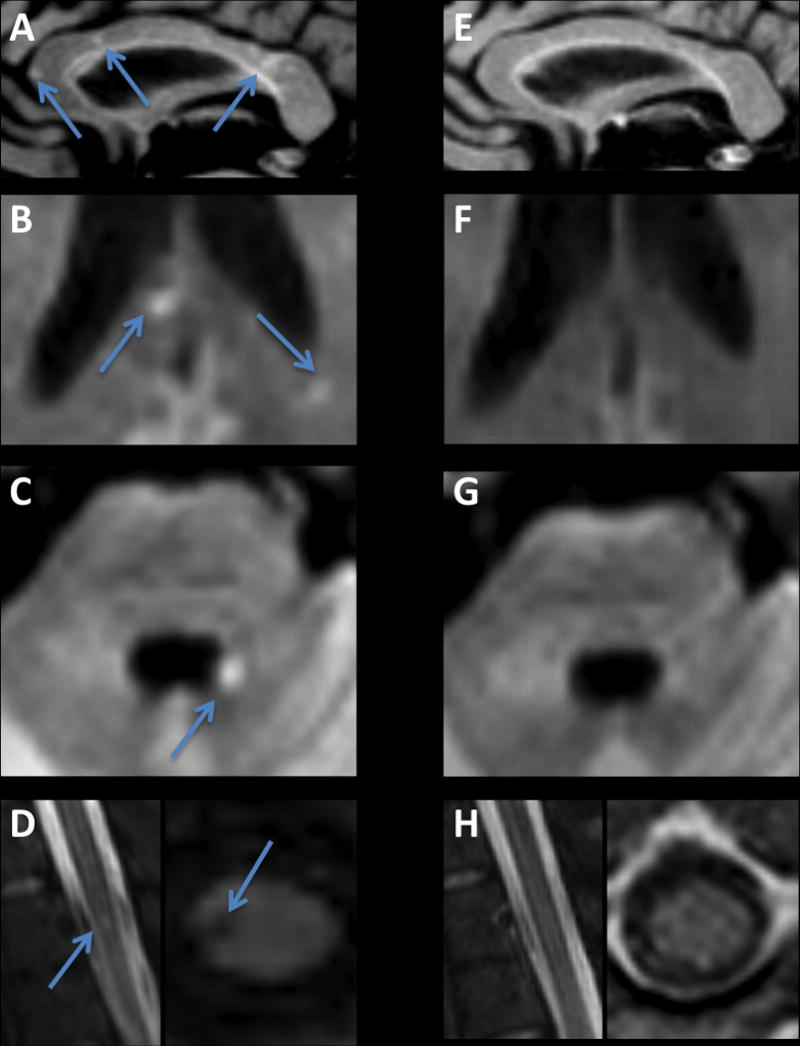
Brain MRI following recovery from Ebola meningoencephalitis: (A–D) Initial MRI, performed on day 33. (A) T2-weighted FLAIR image showing multiple punctate high signal intensity lesions in the corpus callosum. Some of the corpus callosum lesions (B), as well as a lesion on the margin of the fourth ventricle (C), showed restriction of diffusion, compatible with microvascular occlusion and ischemia. (D) A lesion in the right lateral column of the thoracic spinal cord. (E–H)
References
-
- Chertow DS, Kleine C, Edwards JK, Scaini R, Giuliani R, Sprecher A. Ebola virus disease in West Africa–clinical manifestations and management. N Engl - PubMed
-
- World Health Organization. Ebola situation report-21 October 2015. http://apps.who.int/ebola/current-situation/ebola-situation-report-21-oc... (Accessed on October 23, 2015)
-
- Howlett P, Brown C, Helderman T, Brooks T, Lisk D, Deen G, et al. Ebola virus disease complicated by late-onset encephalitis and polyarthritis, Sierra Leone [letter] Emerg Infect Dis. 2016 Jan; (Cited November 11, 2015). http://dx.doi.org/10.3201/eid2201.151212. - DOI - PMC - PubMed
-
- Bechtelsheimer H, Korb G, Gedigk P. The “Marburg-virus”-hepatitis. Studies in man and guinea pigs. Virchows Arch A Pathol Pathol Anat. 1970;351:273–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical