

Phenotypic Variability of Childhood Charcot-Marie-Tooth Disease
- PMID: 27043305
- PMCID: PMC4916861
- DOI: 10.1001/jamaneurol.2016.0171
Phenotypic Variability of Childhood Charcot-Marie-Tooth Disease
Abstract
Importance: Disease severity of childhood Charcot-Marie-Tooth disease (CMT) has not been extensively characterized, either within or between types of CMT to date.
Objective: To assess the variability of disease severity in a large cohort of children and adolescents with CMT.
Design, setting, and participants: A cross-sectional study was conducted among 520 children and adolescents aged 3 to 20 years at 8 universities and hospitals involved in the Inherited Neuropathies Consortium between August 6, 2009, and July 31, 2014, in Australia, Italy, the United Kingdom, and the United States. Data analysis was conducted from August 1, 2014, to December 1, 2015.
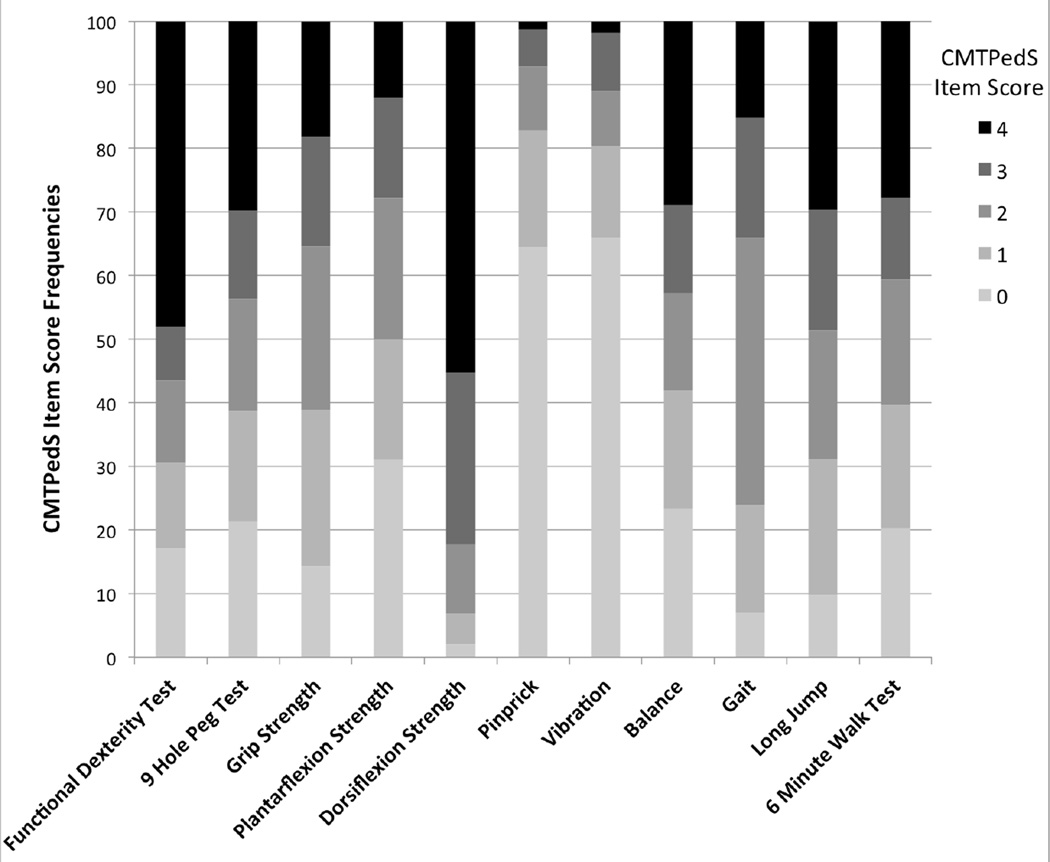
Main outcomes and measures: Scores on the Charcot-Marie-Tooth Disease Pediatric Scale (CMTPedS), a well-validated unidimensional clinical outcome measure to assess disease severity. This instrument includes 11 items assessing fine and gross motor function, sensation, and balance to produce a total score ranging from 0 (unaffected) to 44 (severely affected).
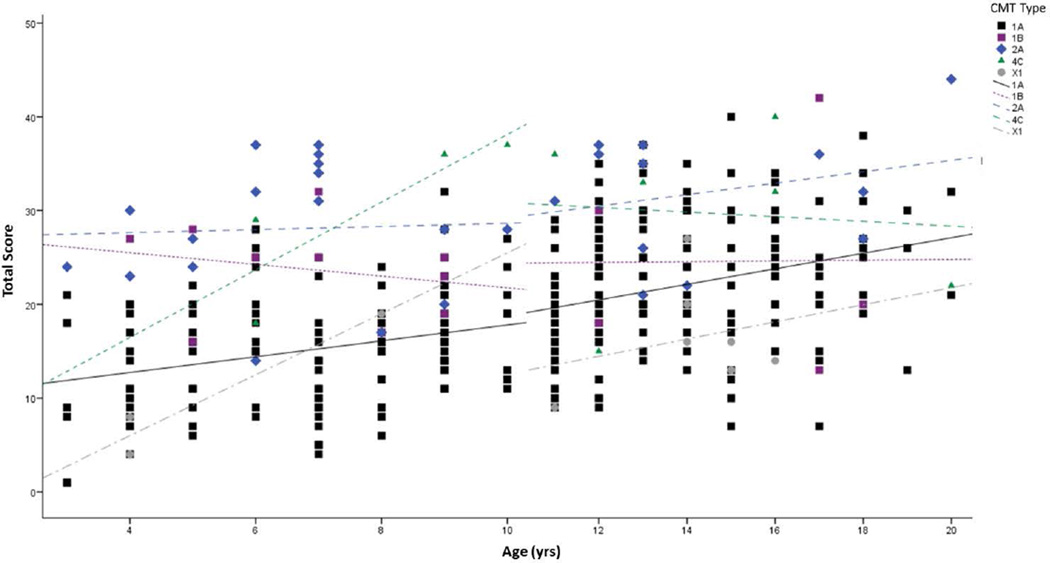
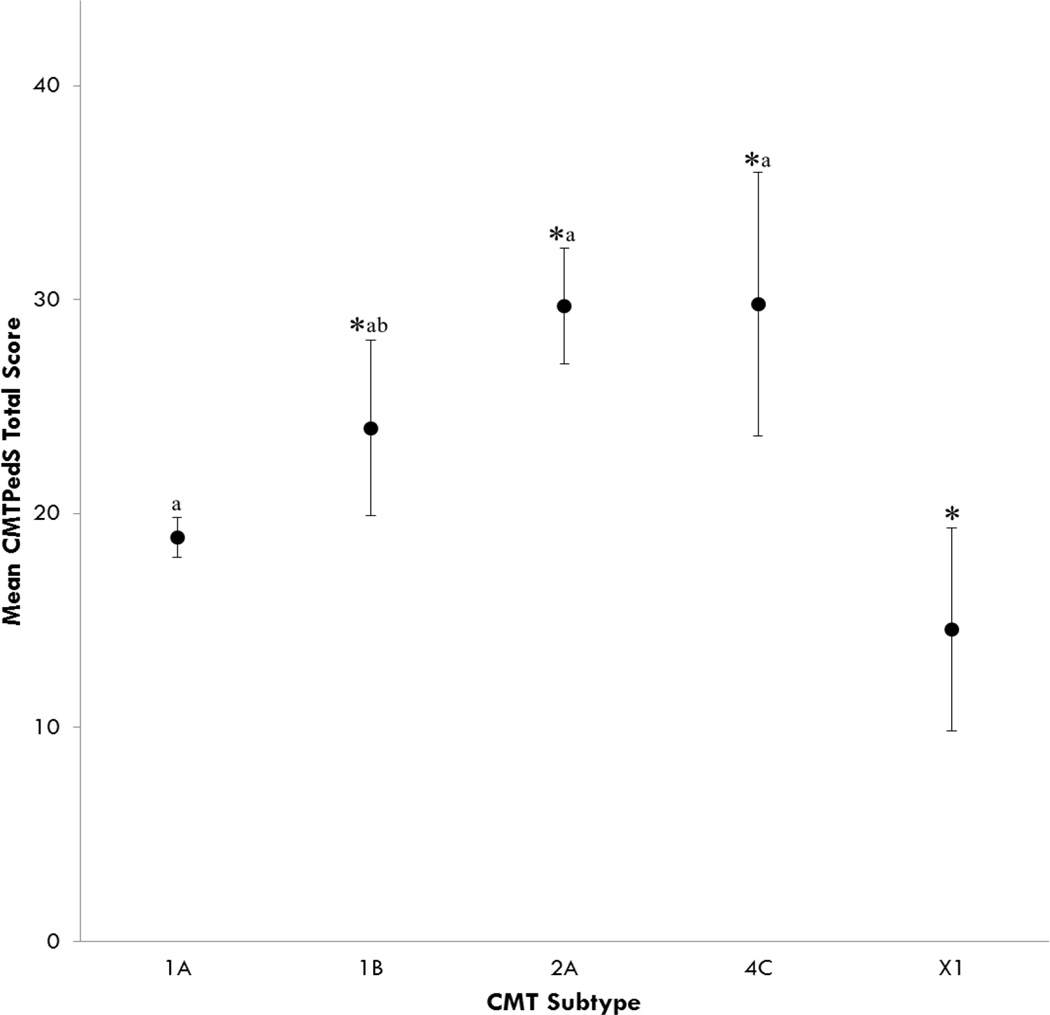
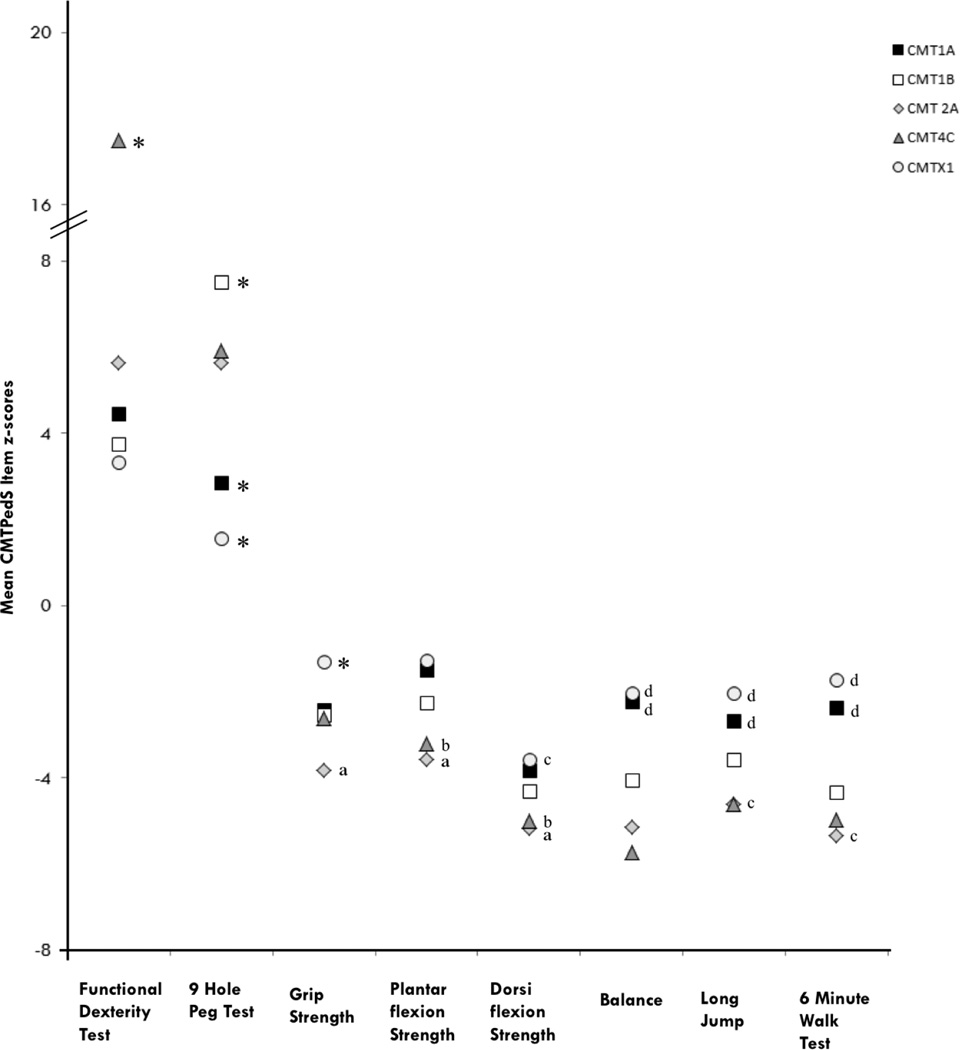
Results: Among the 520 participants (274 males) aged 3 to 20 years, CMT type 1A (CMT1A) was the most prevalent type (252 [48.5%]), followed by CMT2A (31 [6.0%]), CMT1B (15 [2.9%]), CMT4C (13 [2.5%]), and CMTX1 (10 [1.9%]). Disease severity ranged from 1 to 44 points on the CMTPedS (mean [SD], 21.5 [8.9]), with ankle dorsiflexion strength and functional hand dexterity test being most affected. Participants with CMT1B (mean [SD] CMTPedS score, 24.0 [7.4]), CMT2A (29.7 [7.1]), and CMT4C (29.8 [8.6]) were more severely affected than those with CMT1A (18.9 [7.7]) and CMTX1 (males: 15.3 [7.7]; females: 13.0 [3.6]) (P < .05). Scores on the CMTPedS tended to worsen principally during childhood (ages, 3-10 years) for participants with CMT4C and CMTX1 and predominantly during adolescence for those with CMT1B and CMT2A (ages, 11-20 years), while CMT1A worsened consistently throughout childhood and adolescence. For individual items, participants with CMT4C recorded more affected functional dexterity test scores than did those with all other types of CMT (P < .05). Participants with CMT1A and CMTX1 performed significantly better on the 9-hole peg test and balance test than did those with all other types of CMT (P < .05). Participants with CMT2A had the weakest grip strength (P < .05), while those with CMT2A and CMT4C exhibited the weakest ankle plantarflexion and dorsiflexion strength, as well as the lowest long jump and 6-minute walk test distances (P < .05). Multiple regression modeling identified increasing age (r = 0.356, β = 0.617, P < .001) height (r = 0.251, β = 0.309, P = .002), self-reported foot pain (r = 0.162, β = .114, P = .009), and self-reported hand weakness (r = 0.243, β = 0.203, P < .001) as independent predictors of disease severity.
Conclusions and relevance: These results highlight the phenotypic variability within CMT genotypes and mutation-specific manifestations between types. This study has identified distinct functional limitations and self-reported impairments to target in future therapeutic trials.
Conflict of interest statement
Figures
Comment in
-
Precision Medicine for Charcot-Marie-Tooth Disease.JAMA Neurol. 2016 Jun 1;73(6):623-4. doi: 10.1001/jamaneurol.2016.0285. JAMA Neurol. 2016. PMID: 27042938 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
