

Effects of full-neck volumetric-modulated arc therapy vs split-field intensity-modulated head and neck radiation therapy on low neck targets and structures
- PMID: 27043353
- PMCID: PMC5258173
- DOI: 10.1259/bjr.20160009
Effects of full-neck volumetric-modulated arc therapy vs split-field intensity-modulated head and neck radiation therapy on low neck targets and structures
Abstract
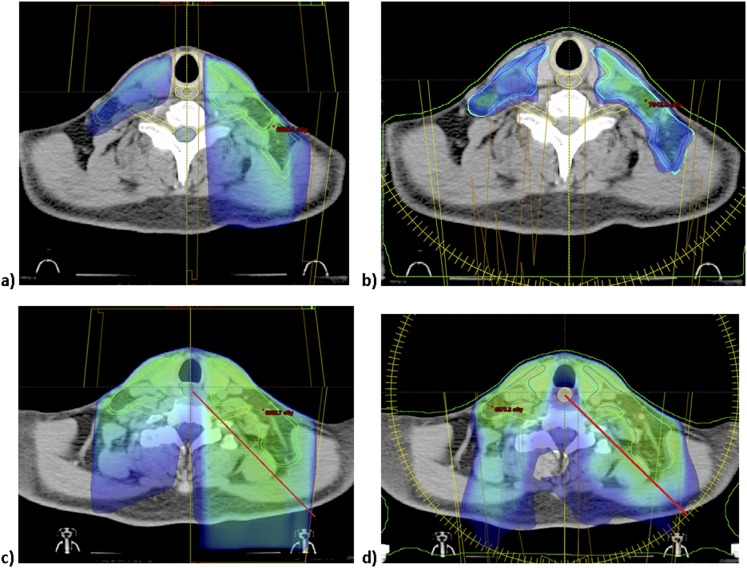
Objective: While split-field intensity-modulated radiation therapy (SF-IMRT) decreases dose to low neck (LAN) structures such as the glottic larynx compared with full-neck intensity-modulated radiation therapy (IMRT), it is unknown whether SF-IMRT affords superior dose avoidance to organs than whole neck-field volumetric-modulated arc therapy (WF-VMAT).
Methods: 10 patients treated definitively with radiation for oropharyngeal, oral cavity or nasopharyngeal carcinoma were compared. Only patients ideally suited for SF-IMRT plans were included. The glottic larynx, supraglottic larynx, arytenoids, pharyngeal constrictors, oesophagus, brachial plexus and target volume coverage in the LAN were compared between WF-VMAT and SF-IMRT.
Results: Volumetric-modulated arc therapy (VMAT) yielded statistically significant decreases in maximum dose to the arytenoids and mean dose to the oesophagus. There was no difference in dose to the glottic larynx, supraglottic larynx, pharyngeal constrictors and brachial plexus. WF-VMAT led to improved coverage to 50/2 Gy fraction equivalent in LAN compared with SF-IMRT using an anteroposterior (AP) LAN field but no difference to the 60/2 Gy fraction equivalent between SF-IMRT and WF-VMAT using AP/posterior-anterior LAN boost.
Conclusion: WF-VMAT affords equivalent glottic and supraglottic larynx dose and lower dose to the arytenoids and oesophagus. WF-VMAT better covers most LAN target structures. Given these findings as well as concerns with matchline cold spots or hotspots with SF-IMRT, patients requiring comprehensive elective nodal irradiation should typically be treated with WF-VMAT.
Advances in knowledge: SF-IMRT for larynx sparing has better dosimetric results to normal structures than whole-neck IMRT, but with increased matchline recurrence risk. We show dosimetric equivalence or superiority of WF-VMAT compared with SF-IMRT.
Figures
References
-
- Nutting CM, Morden JP, Harrington KJ, Urbano TG, Bhide SA, Clark C, et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol 2011; 12: 127–36. doi: 10.1016/S1470-2045(10)70290-4 - DOI - PMC - PubMed
-
- Vanetti E, Clivio A, Nicolini G, Fogliata A, Ghosh-Laskar S, Agarwal JP, et al. Volumetric modulated arc radiotherapy for carcinomas of the oro-pharynx, hypo-pharynx and larynx: a treatment planning comparison with fixed field IMRT. Radiother Oncol 2009; 92: 111–7. doi: 10.1016/j.radonc.2008.12.008 - DOI - PubMed
-
- Grégoire V, Ang K, Budach W, Grau C, Hamoir M, Langendijk JA, et al. Delineation of the neck node levels for head and neck tumors: a 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiother Oncol 2014; 110: 172–81. doi: 10.1016/j.radonc.2013.10.010 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
