

Certain Autoimmune Manifestations Are Associated With Distinctive Karyotypes and Outcomes in Patients With Myelodysplastic Syndrome: A Retrospective Cohort Study
- PMID: 27043672
- PMCID: PMC4998533
- DOI: 10.1097/MD.0000000000003091
Certain Autoimmune Manifestations Are Associated With Distinctive Karyotypes and Outcomes in Patients With Myelodysplastic Syndrome: A Retrospective Cohort Study
Abstract
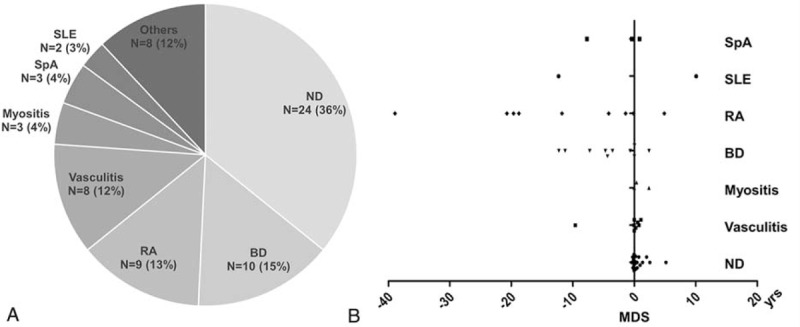
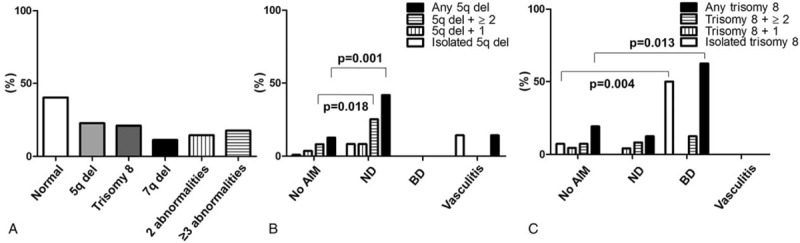
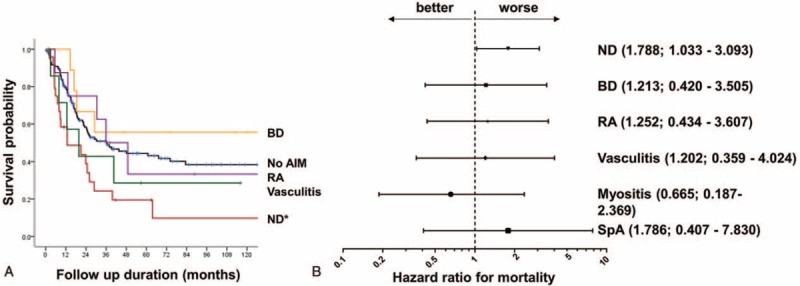
Autoimmune manifestations (AIMs) are common in patients with myelodysplastic syndrome (MDS). This study aimed to investigate whether AIMs are associated with a specific cytogenetic abnormalities and worse survival in patients with MDS. A total of 67 MDS patients with AIMs and 134 age- and sex-matched MDS patients without AIMs, all of whom received medical care at Seoul National University Hospital from January 2000 through July 2014, were enrolled. The clinical features, chromosomal abnormalities, and outcomes were examined. The effect of AIMs on mortality was estimated after adjusting for age, sex, and the International Prognostic Scoring System. The mean age (±SD) at the time of MDS diagnosis was 54.5 ± 17.1 years, and 44.8% of patients were male. Neutrophilic dermatosis (ND; Sweet syndrome and pyoderma gangrenosum) was the most prevalent AIM (n = 24 36%]), followed by Behcet disease (10 [15%]), rheumatoid arthritis (9 [13%]), vasculitis (8 [12%]), myositis (3 [4%]), spondyloarthropathy (3 [4%]), and systemic lupus erythematous (2 [3%]). ND and vasculitis occurred at the time of MDS diagnosis, whereas other AIMs occurred years after MDS diagnosis. Deletion of 5q was associated with ND (P = 0.001), whereas trisomy 8 was associated with Behcet disease (P = 0.015). Strikingly, ND was associated with a 1.8-fold increase in mortality (95% CI 1.033-3.093; P = 0.038). Certain AIMs in MDS patients are associated with distinctive karyotypes and worse survival. A larger study is needed to confirm whether the presence of AIMs influences disease outcome in MDS.
Conflict of interest statement
The authors have no competing interests to declare. The authors have no conflicts of interest to disclose.
Figures
References
-
- Albitar M, Manshouri T, Shen Y, et al. Myelodysplastic syndrome is not merely “preleukemia”. Blood 2002; 100:791–798. - PubMed
-
- Enright H, Jacob HS, Vercellotti G, et al. Paraneoplastic autoimmune phenomena in patients with myelodysplastic syndromes: response to immunosuppressive therapy. Br J Haematol 1995; 91:403–408. - PubMed
-
- Okamoto T, Okada M, Mori A, et al. Correlation between immunological abnormalities and prognosis in myelodysplastic syndrome patients. Int J Hematol 1997; 66:345–351. - PubMed
-
- Marisavljevic D, Kraguljac N, Rolovic Z. Immunologic abnormalities in myelodysplastic syndromes: clinical features and characteristics of the lymphoid population. Med Oncol 2006; 23:385–391. - PubMed
-
- Giannouli S, Voulgarelis M, Zintzaras E, et al. Autoimmune phenomena in myelodysplastic syndromes: a 4-yr prospective study. Rheumatology (Oxford) 2004; 43:626–632. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
