

Dilemma of managing asymptomatic children referred with 'culture-confirmed' drug-resistant tuberculosis
- PMID: 27044259
- PMCID: PMC4996348
- DOI: 10.1136/archdischild-2015-310186
Dilemma of managing asymptomatic children referred with 'culture-confirmed' drug-resistant tuberculosis
Abstract
Background: The diagnosis of drug-resistant tuberculosis (DR-TB) in children is challenging and treatment is associated with many adverse effects.
Objective: We aimed to assess if careful observation, without initiation of second-line treatment, is safe in asymptomatic children referred with 'culture-confirmed' DR-TB.
Setting: KwaZulu-Natal, South Africa-an area with high burdens of HIV, TB and DR-TB.
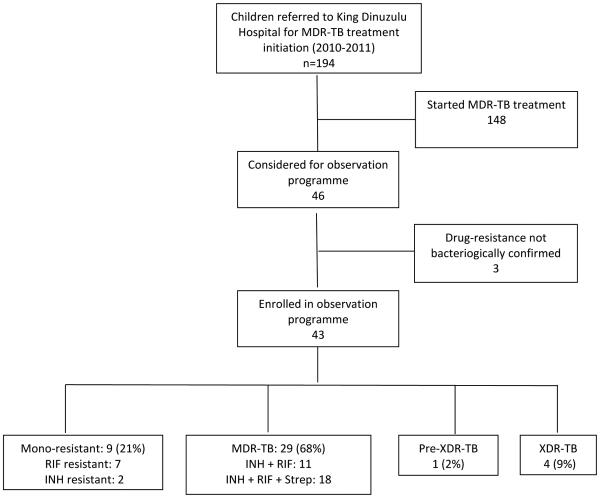
Design, intervention and main outcome measures: We performed an outcome review of children with 'culture-confirmed' DR-TB who were not initiated on second-line TB treatment, as they were asymptomatic with normal chest radiographs on examination at our specialist referral hospital. Children were followed up every other month for the first year, with a final outcome assessment at the end of the study.
Results: In total, 43 asymptomatic children with normal chest radiographs were reviewed. The median length of follow-up until final evaluation was 549 days (IQR 259-722 days); most (34; 83%) children were HIV uninfected. Resistance patterns included 9 (21%) monoresistant and 34 (79%) multidrug-resistant (MDR) strains. Fifteen children (35%) had been treated with first-line TB treatment, prior to presentation at our referral hospital. At the final evaluation, 34 (80%) children were well, 7 (16%) were lost to follow-up, 1 (2%) received MDR-TB treatment and 1 (2%) died of unknown causes. The child who received MDR-TB treatment developed new symptoms at the 12-month review and responded well to second-line treatment.
Conclusions: Bacteriological evaluation should not be performed in the absence of any clinical indication. If drug-resistant Mycobacterium tuberculosis is detected in an asymptomatic child with a normal chest radiograph, close observation may be an appropriate strategy, especially in settings where potential laboratory error and poor record keeping are constant challenges.
Keywords: Asymptomatic; DR-TB; HIV; children; management.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Comment in
-
Two sizes do not fit all: the terms infection and disease are inadequate for the description of children with tuberculosis.Arch Dis Child. 2016 Jul;101(7):594-5. doi: 10.1136/archdischild-2016-310747. Epub 2016 May 11. Arch Dis Child. 2016. PMID: 27169765 No abstract available.
References
-
- World Health Organization . WHO/HTM/TB/2015.22. World Health Organisation; Geneva, Switzerland: 2015. Global tuberculosis report 2015. (http://www.who.int/tb/publications/global_report/en/)
-
- Seddon J, Hesseling A, Willemse M, et al. Culture-confirmed multidrug-resistant tuberculosis in children: clinical features, treatment, and outcome. Clin Infect Dis. 2012;54:157–66. - PubMed
-
- Beyers N, Gie R, Schaaf H, et al. Delay in the diagnosis, notification and initiation of treatment and compliance in children with tuberculosis. Tubercle and Lung Disease. 1994;75:260–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical