

Preeclampsia and toxic metals: a case-control study in Kinshasa, DR Congo
- PMID: 27044488
- PMCID: PMC4820935
- DOI: 10.1186/s12940-016-0132-1
Preeclampsia and toxic metals: a case-control study in Kinshasa, DR Congo
Abstract
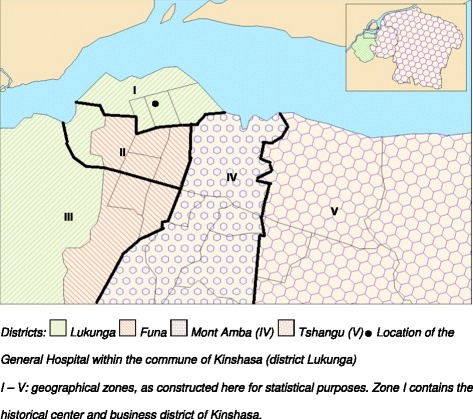
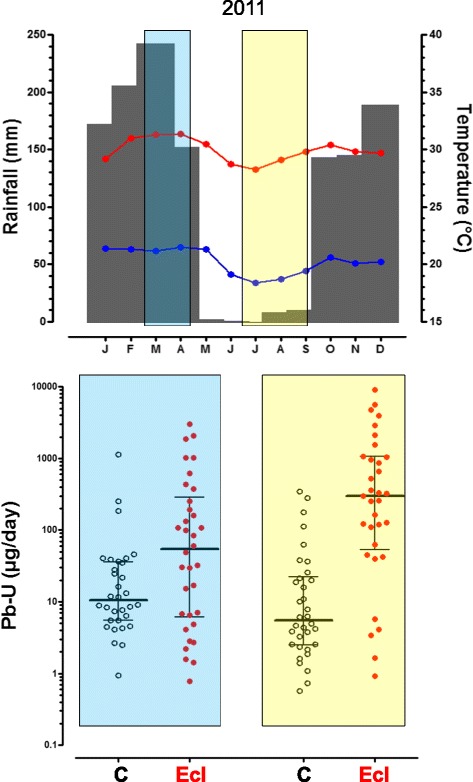
Background: Preeclampsia is frequent in Kinshasa (Democratic Republic of Congo), especially during the dry season. We tested whether preeclampsia was associated with exposure to environmental metals.
Methods: Using a case-control design, 88 women hospitalized with preeclampsia (cases) and 88 healthy pregnant women from the antenatal clinic (controls) were included in the study; 67 and 109 women were enrolled during the rainy and dry season, respectively. The concentrations of 24 elements were quantified by inductively coupled plasma mass spectrometry (ICP-MS) in 24-h urine collections. Differences in the urinary excretion of metals were investigated between cases and controls, and the interaction with season was assessed.
Results: Cases and controls were well matched regarding age, parity and duration of pregnancy. In controls, the urinary concentrations of most elements were substantially higher than reference values for adults from industrially developed countries, e.g. for lead: geometric mean (GM) 8.0 μg/L [25(th)-75(th) percentile 3.1-13.8]. The daily urinary excretions of 14 metals were significantly higher in women with preeclampsia than in control women, e.g. for lead: GM 61 μg/day (25(th)-75(th) percentile 8-345) in women with preeclampsia vs 9 μg/day (25(th)-75(th) percentile 3-21) in controls (p < 0.001). A significant interaction was found between season and preeclampsia for several elements, with higher urinary excretions in preeclamptic women than controls during the dry season, but not during the rainy season.
Conclusions: This study revealed not only that women with preeclampsia excrete higher amounts of several toxic metals, especially lead, than control women, but also that this excretion exhibits seasonal variation, thus possibly explaining the high incidence and seasonal variation of preeclampsia in Kinshasa. Although the exact sources of this exposure are unknown, these findings underscore the need for preventing environmental exposures to lead and other toxic metals.
Keywords: Developing country; Global health; Hypertension; Lead; Metal pollution; Preeclampsia; Seasonality.
Figures
Similar articles
-
Urinary concentrations of environmental metals and associating factors in pregnant women.Environ Sci Pollut Res Int. 2019 May;26(13):13464-13475. doi: 10.1007/s11356-019-04731-z. Epub 2019 Mar 25. Environ Sci Pollut Res Int. 2019. PMID: 30911968
-
High human exposure to cobalt and other metals in Katanga, a mining area of the Democratic Republic of Congo.Environ Res. 2009 Aug;109(6):745-52. doi: 10.1016/j.envres.2009.04.012. Epub 2009 May 31. Environ Res. 2009. PMID: 19486963
-
Current exposure to environmental pollutants in the general adult population of Kinshasa, Democratic Republic of Congo (DRC): A cross-sectional study.Int J Hyg Environ Health. 2025 Jan;263:114479. doi: 10.1016/j.ijheh.2024.114479. Epub 2024 Oct 13. Int J Hyg Environ Health. 2025. PMID: 39405608
-
Assessing exposure to metals using biomonitoring: Achievements and challenges experienced through surveys in low- and middle-income countries.Toxicol Lett. 2018 Dec 1;298:13-18. doi: 10.1016/j.toxlet.2018.06.004. Epub 2018 Jun 9. Toxicol Lett. 2018. PMID: 29894842 Review.
-
A global perspective of correlation between maternal blood lead levels and risks of preeclampsia: An updated systematic review and meta-analysis.Front Public Health. 2022 Dec 23;10:1072052. doi: 10.3389/fpubh.2022.1072052. eCollection 2022. Front Public Health. 2022. PMID: 36620238 Free PMC article.
Cited by
-
A cross-sectional examination of the early-onset hypertensive disorders of pregnancy and industrial emissions of toxic metals using Kentucky birth records, 2008-2017.PLoS One. 2022 Sep 20;17(9):e0274250. doi: 10.1371/journal.pone.0274250. eCollection 2022. PLoS One. 2022. PMID: 36125992 Free PMC article.
-
Urinary concentrations of environmental metals and associating factors in pregnant women.Environ Sci Pollut Res Int. 2019 May;26(13):13464-13475. doi: 10.1007/s11356-019-04731-z. Epub 2019 Mar 25. Environ Sci Pollut Res Int. 2019. PMID: 30911968
-
Association between prenatal arsenic exposure, birth outcomes, and pregnancy complications: An observational study within the National Children's Study cohort.Environ Res. 2020 Apr;183:109182. doi: 10.1016/j.envres.2020.109182. Epub 2020 Jan 24. Environ Res. 2020. PMID: 32058141 Free PMC article.
-
Exposure to Metal Mixtures in Association with Cardiovascular Risk Factors and Outcomes: A Scoping Review.Toxics. 2022 Mar 1;10(3):116. doi: 10.3390/toxics10030116. Toxics. 2022. PMID: 35324741 Free PMC article.
-
Environmental Toxicant Exposure and Hypertensive Disorders of Pregnancy: Recent Findings.Curr Hypertens Rep. 2018 Aug 8;20(10):87. doi: 10.1007/s11906-018-0888-5. Curr Hypertens Rep. 2018. PMID: 30090982 Free PMC article. Review.
References
-
- Elongi JP, Tandu B, Spitz B, Verdonck F. Influence de la variation saisonnière sur la prévalence de la pré-éclampsie à Kinshasa [Influence of the seasonal variation on the prevalence of pre-eclampsia in Kinshasa] Gynecol Obstet Fertil. 2011;39:132–5. doi: 10.1016/j.gyobfe.2010.12.010. - DOI - PubMed
-
- Elongi JP, Bamba D, Tandu U, Spitz B, Verdonck F, Dikamba N. Appréciation de la consommation des légumes verts et fruits chez les gestantes à Kinshasa [Estimated consumption of green vegetables and fruit among pregnant women in Kinshasa]. Médecine d'Afrique noire 2011; N° 5803:115-121.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
