

Genital invasion or perigenital spread may pose a risk of marginal misses for Intensity Modulated Radiotherapy (IMRT) in anal cancer
- PMID: 27044498
- PMCID: PMC4820940
- DOI: 10.1186/s13014-016-0628-4
Genital invasion or perigenital spread may pose a risk of marginal misses for Intensity Modulated Radiotherapy (IMRT) in anal cancer
Abstract
Background: While intensity modulated radiotherapy (IMRT) in anal cancer is feasible and improves high-dose conformality, the current RTOG/AGITG contouring atlas and planning guidelines lack specific instructions on how to proceed with external genitalia. Meanwhile, the RTOG-Protocol 0529 explicitly recommends genital sparing on the basis of specific genital dose constraints. Recent pattern-of-relapse studies based on conventional techniques suggest that marginal miss might be a potential consequence of genital sparing. Our goal is to outline the potential scope and increase the awareness for this clinical issue.
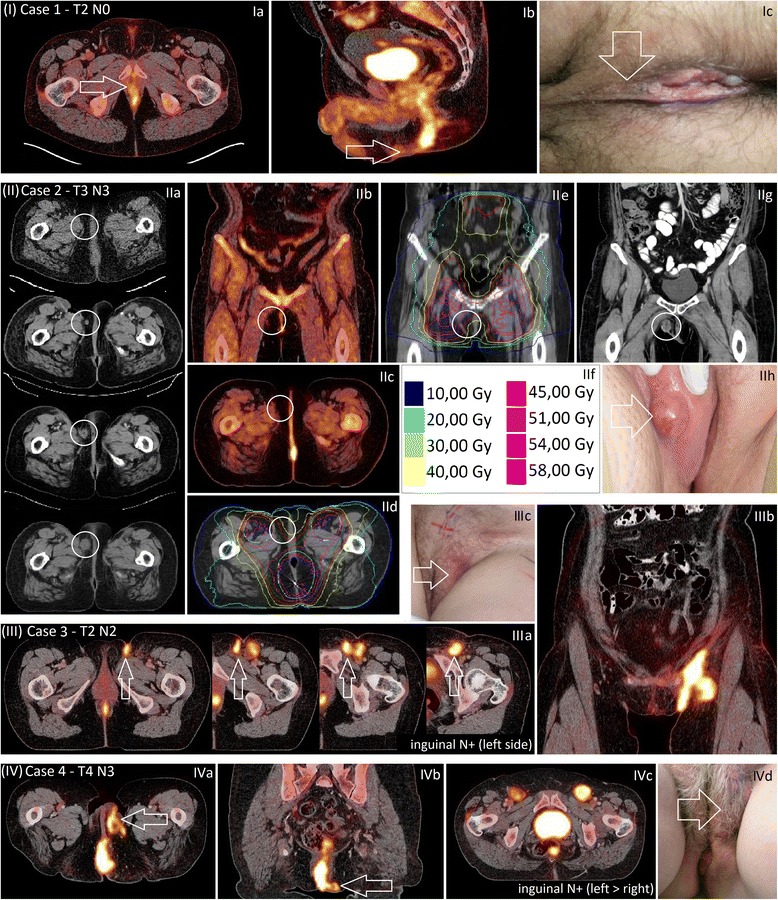
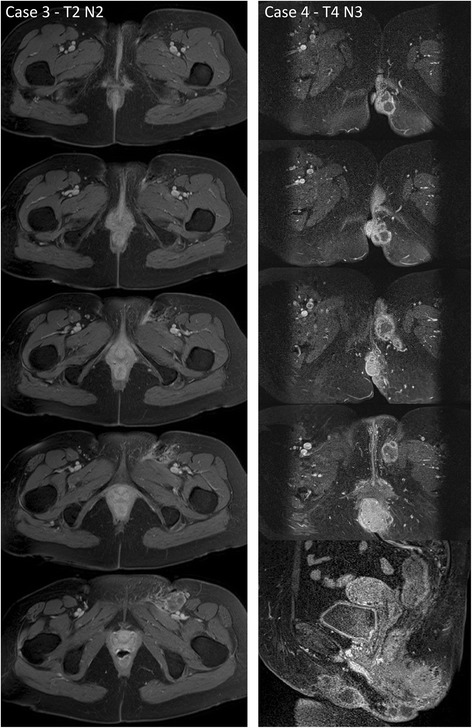
Methods: We present and discuss four patients with perigenital spread in anal cancer in both early and advanced stages (three at time of first diagnosis and one in form of relapse). Genital/perigenital spread was observed once as direct genital infiltration and thrice in form of perigenital lymphatic spread.
Results: We review the available data regarding the potential consequences of genital sparing in anal cancer. Pattern-of-relapse studies in anal cancer after conventional radiotherapy and the current use of IMRT in anal cancer are equivocal but suggest that genital sparing may occasionally result in marginal miss. An obvious hypothesis suggested by our report is that perigenital lymphovascular invasion might be associated with manifest inguinal N+ disease.
Conclusions: Local failure has low salvage rates in recent anal cancer treatment series. Perigenital spread may pose a risk of marginal misses in IMRT in anal cancer. To prevent marginal misses, meticulous pattern-of-relapse analyses of controlled IMRT-series are warranted. Until their publication, genital sparing should be applied with caution, PET/CT should be used when possible and meeting genital dose constraints should not be prioritized over CTV coverage, especially (but not only) in stage T3/4 and N+ disease.
Keywords: Anal carcinoma; Genital sparing; Intensity Modulated Radiotherapy (IMRT); Lymphatic spread; Marginal miss; Perigenital spread; Vulvar relapse.
Figures
Similar articles
-
Genital marginal failures after intensity-modulated radiation therapy (IMRT) in squamous cell anal cancer: no higher risk with IMRT when compared to 3DCRT.Med Oncol. 2018 Mar 28;35(5):59. doi: 10.1007/s12032-018-1118-3. Med Oncol. 2018. PMID: 29594584
-
Australasian Gastrointestinal Trials Group (AGITG) contouring atlas and planning guidelines for intensity-modulated radiotherapy in anal cancer.Int J Radiat Oncol Biol Phys. 2012 Aug 1;83(5):1455-62. doi: 10.1016/j.ijrobp.2011.12.058. Epub 2012 Mar 6. Int J Radiat Oncol Biol Phys. 2012. PMID: 22401917
-
RTOG 0529: a phase 2 evaluation of dose-painted intensity modulated radiation therapy in combination with 5-fluorouracil and mitomycin-C for the reduction of acute morbidity in carcinoma of the anal canal.Int J Radiat Oncol Biol Phys. 2013 May 1;86(1):27-33. doi: 10.1016/j.ijrobp.2012.09.023. Epub 2012 Nov 12. Int J Radiat Oncol Biol Phys. 2013. PMID: 23154075 Free PMC article. Clinical Trial.
-
Organ-sparing Intensity-modulated radiotherapy for anal cancer using the ACTII schedule: a comparison of conventional and intensity-modulated radiotherapy plans.Clin Oncol (R Coll Radiol). 2013 Mar;25(3):155-61. doi: 10.1016/j.clon.2012.08.008. Epub 2012 Sep 14. Clin Oncol (R Coll Radiol). 2013. PMID: 22981970
-
Elective clinical target volumes for conformal therapy in anorectal cancer: a radiation therapy oncology group consensus panel contouring atlas.Int J Radiat Oncol Biol Phys. 2009 Jul 1;74(3):824-30. doi: 10.1016/j.ijrobp.2008.08.070. Epub 2008 Dec 29. Int J Radiat Oncol Biol Phys. 2009. PMID: 19117696 Free PMC article.
Cited by
-
A Case Report of Locally Advanced Anal Cancer with Solitary Cutaneous Nodular Metastasis in the Ipsilateral Labia Majora Treated with Definitive Chemoradiotherapy.Case Rep Oncol. 2019 Sep 19;12(3):721-727. doi: 10.1159/000503171. eCollection 2019 Sep-Dec. Case Rep Oncol. 2019. PMID: 31607890 Free PMC article.
-
Genital marginal failures after intensity-modulated radiation therapy (IMRT) in squamous cell anal cancer: no higher risk with IMRT when compared to 3DCRT.Med Oncol. 2018 Mar 28;35(5):59. doi: 10.1007/s12032-018-1118-3. Med Oncol. 2018. PMID: 29594584
-
Patterns of recurrence in anal cancer: a detailed analysis.Radiat Oncol. 2020 May 27;15(1):125. doi: 10.1186/s13014-020-01567-7. Radiat Oncol. 2020. PMID: 32460785 Free PMC article.
-
Management of anal cancer patients - a pattern of care analysis in German-speaking countries.Radiat Oncol. 2020 May 25;15(1):122. doi: 10.1186/s13014-020-01539-x. Radiat Oncol. 2020. PMID: 32450863 Free PMC article.
-
Perineal body squamous cell carcinoma treated with radical radiotherapy - a case report.Ecancermedicalscience. 2023 Apr 20;17:1534. doi: 10.3332/ecancer.2023.1534. eCollection 2023. Ecancermedicalscience. 2023. PMID: 37138957 Free PMC article.
References
-
- Bartelink H, Roelofsen F, Eschwege F, Rougier P, Bosset JF, Gonzalez DG, et al. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol. 1997;15(5):2040–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
