

Enhancing Cardiac Rehabilitation With Stress Management Training: A Randomized, Clinical Efficacy Trial
- PMID: 27045127
- PMCID: PMC4824555
- DOI: 10.1161/CIRCULATIONAHA.115.018926
Enhancing Cardiac Rehabilitation With Stress Management Training: A Randomized, Clinical Efficacy Trial
Abstract
Background: Cardiac rehabilitation (CR) is the standard of care for patients with coronary heart disease. Despite considerable epidemiological evidence that high stress is associated with worse health outcomes, stress management training (SMT) is not included routinely as a component of CR.
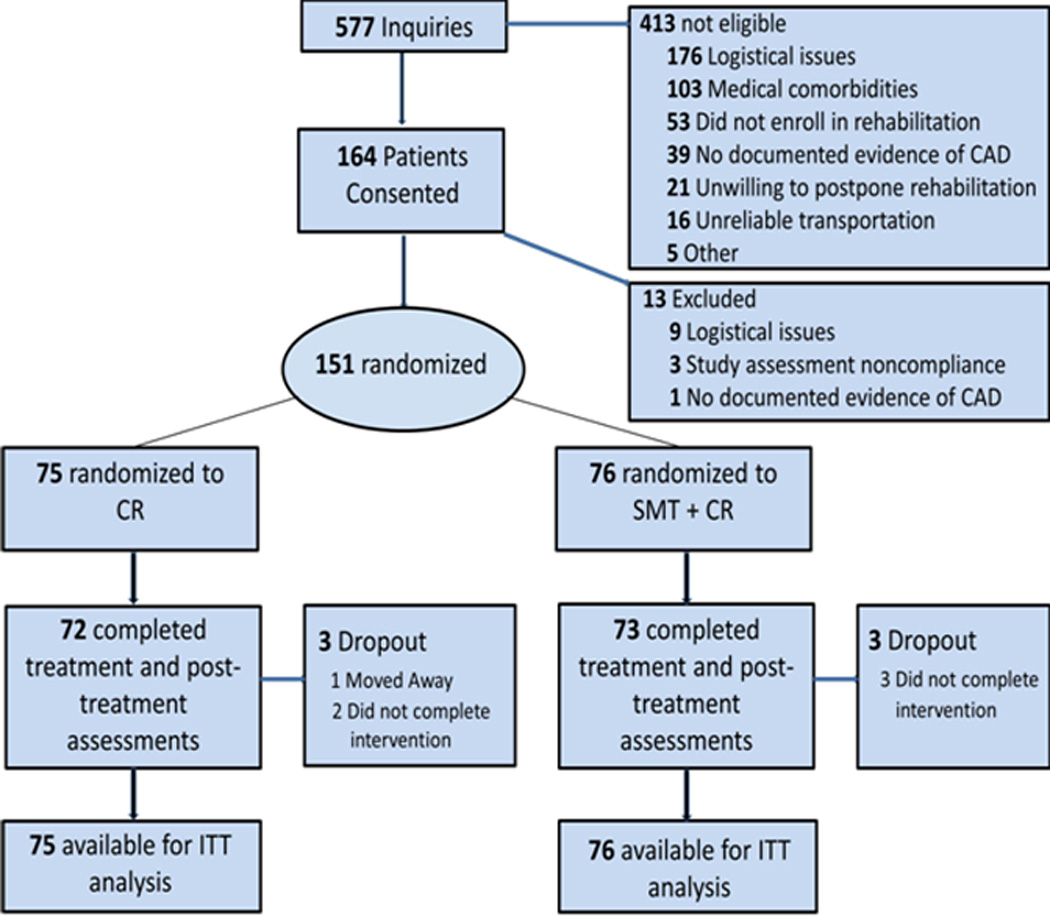
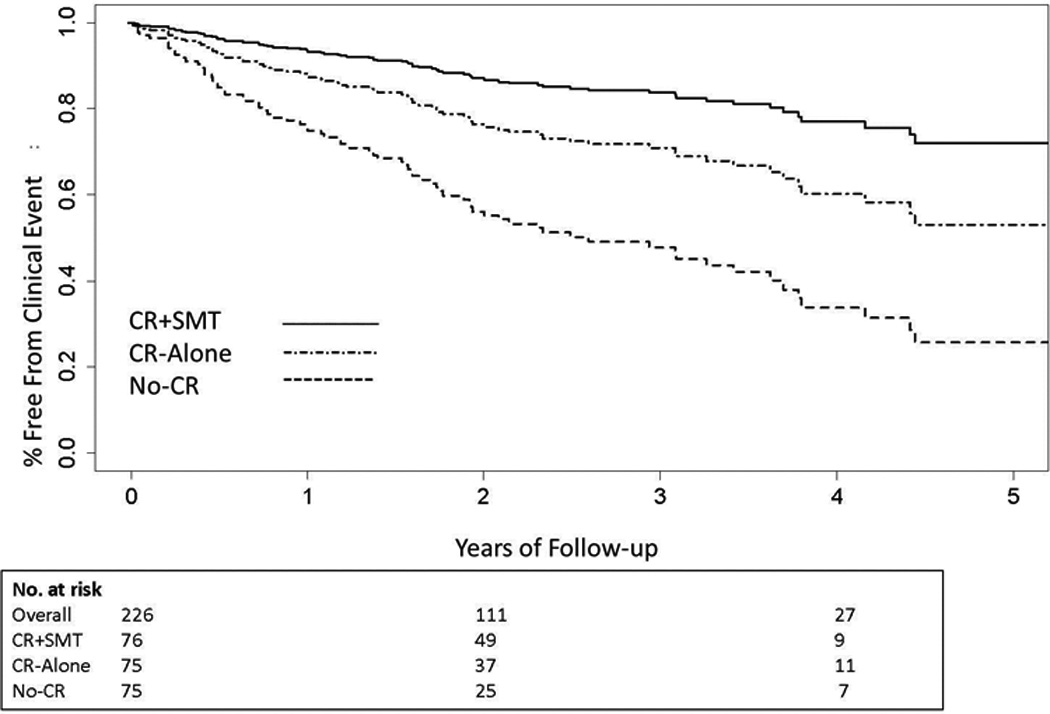
Methods and results: One hundred fifty-one outpatients with coronary heart disease who were 36 to 84 years of age were randomized to 12 weeks of comprehensive CR or comprehensive CR combined with SMT (CR+SMT), with assessments of stress and coronary heart disease biomarkers obtained before and after treatment. A matched sample of CR-eligible patients who did not receive CR made up the no-CR comparison group. All participants were followed up for up to 5.3 years (median, 3.2 years) for clinical events. Patients randomized to CR+SMT exhibited greater reductions in composite stress levels compared with those randomized to CR alone (P=0.022), an effect that was driven primarily by improvements in anxiety, distress, and perceived stress. Both CR groups achieved significant, and comparable, improvements in coronary heart disease biomarkers. Participants in the CR+SMT group exhibited lower rates of clinical events compared with those in the CR-alone group (18% versus 33%; hazard ratio=0.49; 95% confidence interval, 0.25-0.95; P=0.035), and both CR groups had lower event rates compared with the no-CR group (47%; hazard ratio=0.44; 95% confidence interval, 0.27-0.71; P<0.001).
Conclusions: CR enhanced by SMT produced significant reductions in stress and greater improvements in medical outcomes compared with standard CR. Our findings indicate that SMT may provide incremental benefit when combined with comprehensive CR and suggest that SMT should be incorporated routinely into CR.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00981253.
Keywords: coronary disease; epidemiology; exercise; rehabilitation; stress, psychological.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Cardiac rehabilitation: Stress management lowers CHD risk.Nat Rev Cardiol. 2016 May;13(5):248. doi: 10.1038/nrcardio.2016.54. Epub 2016 Apr 7. Nat Rev Cardiol. 2016. PMID: 27053459 No abstract available.
-
Stress management training should be an integral component of cardiac rehabilitation.Evid Based Med. 2017 Apr;22(2):65. doi: 10.1136/ebmed-2016-110532. Epub 2017 Jan 27. Evid Based Med. 2017. PMID: 28130388 No abstract available.
References
-
- Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JA, Franklin B, Sanderson B, Southard D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the american heart association exercise, cardiac rehabilitation, and prevention committee, the council on clinical cardiology; the councils on cardiovascular nursing, epidemiology and prevention, and nutrition, physical activity, and metabolism; and the american association of cardiovascular and pulmonary rehabilitation. Circulation. 2007;115:2675–2682. - PubMed
-
- Ades PA. Cardiac rehabilitation and secondary prevention of coronary heart disease. N Engl J Med. 2001;345:892–902. - PubMed
-
- Anderson L, Oldridge N, Thompson DR, Zwisler A-D, Rees K, Martin N, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart diseasecochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67:1–12. - PubMed
-
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J Am Coll Cardiol. 2005;45:637–651. - PubMed
-
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the interheart study): Case-control study. Lancet. 2004;364:937–952. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
