

Improving Patient Safety Event Reporting Among Residents and Teaching Faculty
- PMID: 27046410
- PMCID: PMC4795509
Improving Patient Safety Event Reporting Among Residents and Teaching Faculty
Abstract
Background: A June 2012 site visit report from the Accreditation Council for Graduate Medical Education Clinical Learning Environment Review revealed that residents and physicians at TriHealth, Inc., a large, nonprofit independent academic medical center serving the Greater Cincinnati area in Ohio, had an opportunity to improve their awareness and understanding of the hospital's system for reporting patient safety concerns in 3 areas: (1) what constitutes a reportable patient safety event, (2) who is responsible for reporting, and (3) how to use the hospital's current reporting system.
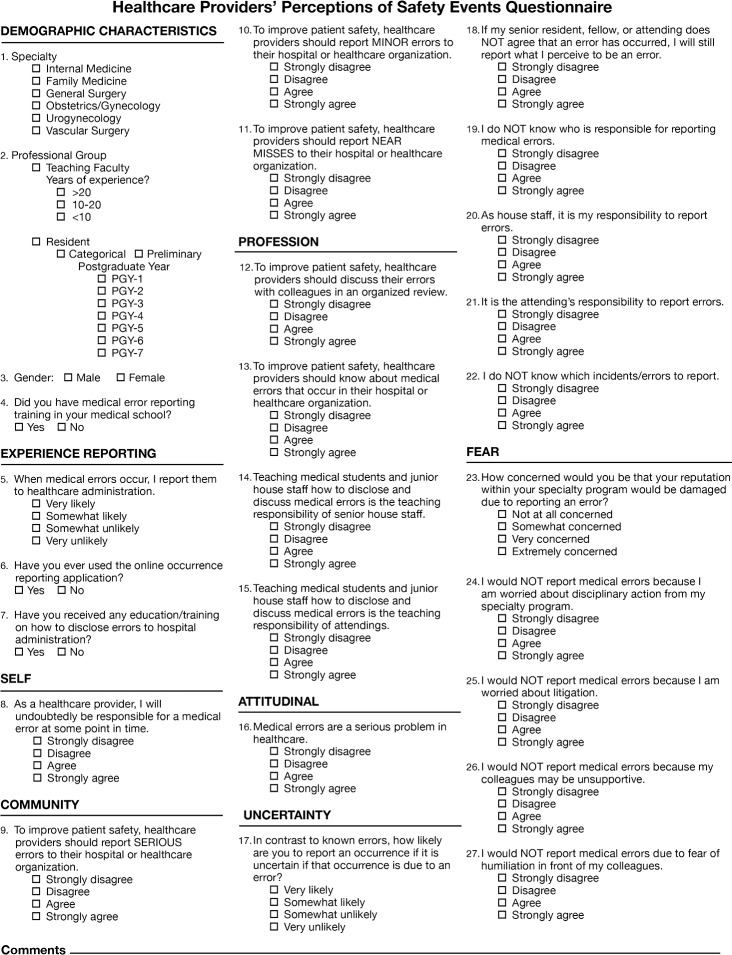
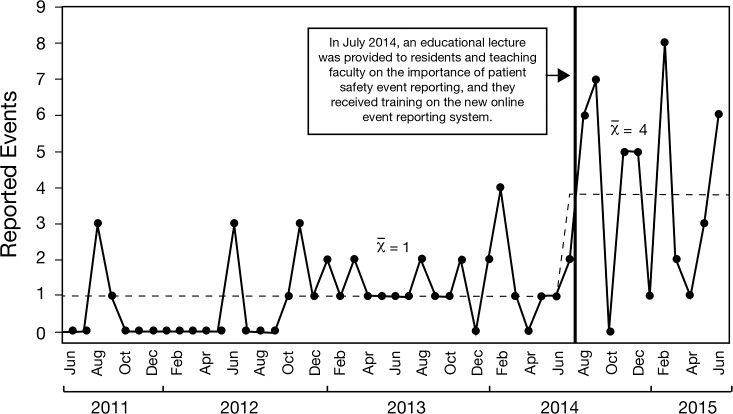
Methods: To improve the culture of patient safety, we designed a quality improvement project with the goal to increase patient safety event reporting among residents and teaching faculty. An anonymous questionnaire assessed physicians' and residents' attitudes and experience regarding patient safety event reporting. An educational intervention was provided in each graduate medical education program to improve knowledge and skills related to patient safety event reporting, and the anonymous questionnaire was distributed after the intervention. We compared the responses to the preintervention and postintervention questionnaires and tracked monthly patient safety event reports for 1 year postintervention.
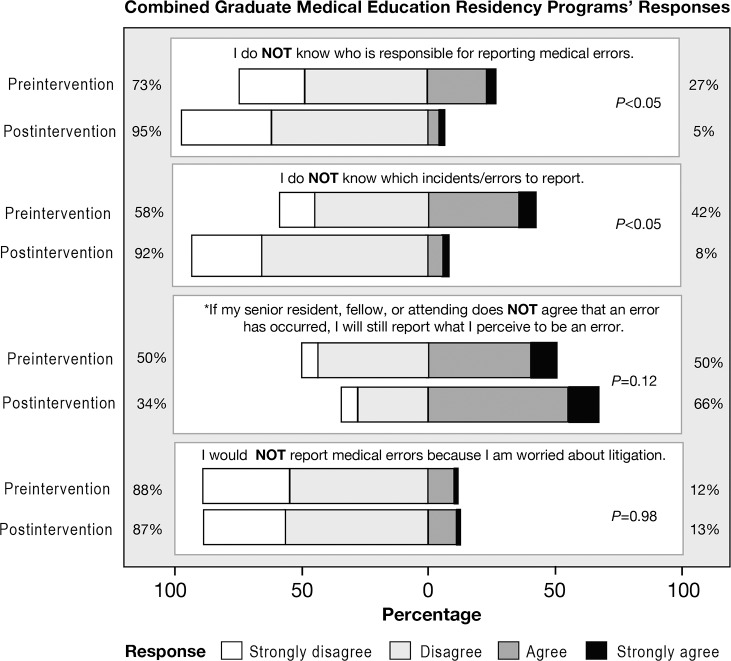
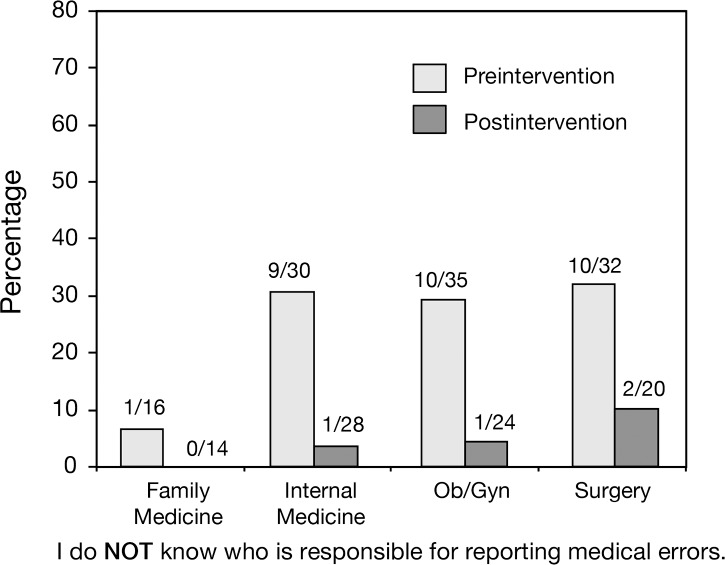
Results: The number of patient safety event reports increased following the educational intervention; however, we saw wide variability in reporting per month. On the postintervention questionnaire, participants demonstrated improved knowledge and attitudes toward patient safety event reporting.
Conclusion: The goal of this unique project was to increase patient safety event reporting by both residents and teaching faculty in 6 residency programs through education. We achieved this goal through an educational intervention tailored to the institution's new event reporting system delivered to each residency program. We clearly understand that improvements in quality and patient safety require ongoing effort. The keys to ongoing sustainability include (1) developing patient safety faculty and resident experts in each training program to teach patient safety and to be role models, (2) working toward decreasing the barriers to reporting, and (3) providing timely feedback and system changes.
Keywords: Education–graduate–medical; hospital incident reporting; medical errors; patient safety; quality improvement; risk management.
Figures

References
-
- Institute of Medicine. To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS. eds Washington, DC: National Academy Press; 1999. - PubMed
-
- Accreditation Council for Graduate Medical Education. ACGME Common Program Requirements; 2013. . https://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/CP.... Accessed November 25, 2015.
LinkOut - more resources
Full Text Sources