

Development and Validation of the Framingham Steatosis Index to Identify Persons With Hepatic Steatosis
- PMID: 27046482
- PMCID: PMC4955680
- DOI: 10.1016/j.cgh.2016.03.034
Development and Validation of the Framingham Steatosis Index to Identify Persons With Hepatic Steatosis
Abstract
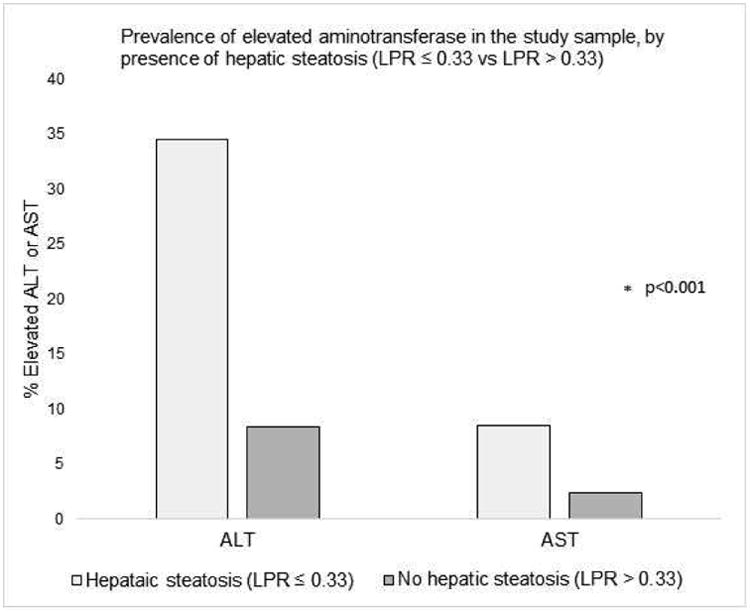
Background & aims: Serum levels of aminotransferases are used as markers of nonalcoholic fatty liver disease in epidemiology research. However, it is not clear whether they can be used to identify patients with fatty liver. We investigated the accuracy of serum levels of aminotransferases in detection of hepatic steatosis. In addition, we derived a Framingham steatosis index (FSI) and tested its ability to identify patients with hepatic steatosis in an independent cohort.
Methods: We performed a cross-sectional study of 1181 members of the Framingham Third Generation Cohort (46.1% women; mean age, 50.3 ± 6.7 years). People with hepatic steatosis were identified by computed tomography that was performed from 2008 through 2011. We compared the abilities of levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) and the ratio of ALT:AST to identify people with hepatic steatosis by using c-statistic analyses. We performed a stepwise regression procedure to identify demographic and clinical factors that correlated with hepatic steatosis; we used these, along with biochemical factors associated with steatosis, to develop the FSI. We validated the FSI by using data from the third National Health and Nutrition Examination Survey.
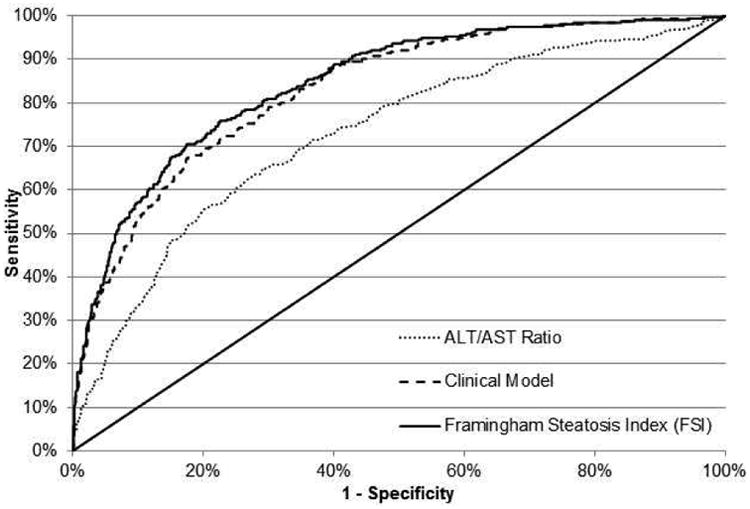
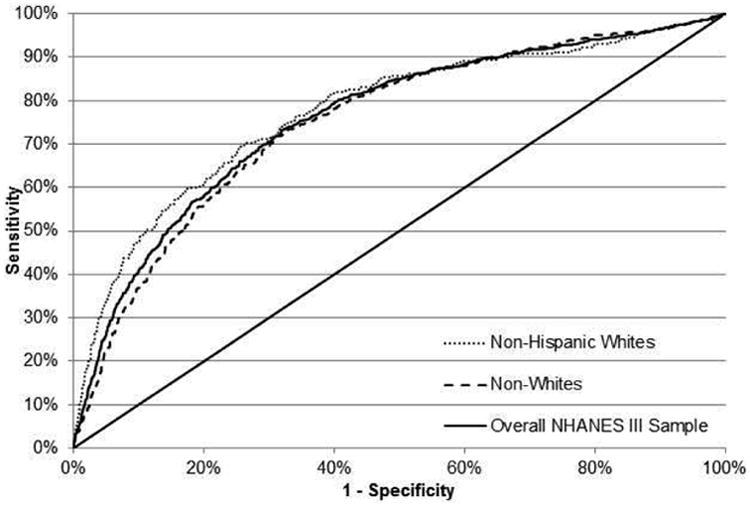
Results: The prevalence of hepatic steatosis in the Framingham Third Generation Cohort was 26.8%. The ratio of ALT:AST identified people with hepatic steatosis with the highest c-statistic value (0.728); the value for only ALT was 0.706, and the value for only AST was 0.589. We derived the FSI on the basis of patient age, sex, body mass index, levels of triglycerides, hypertension, diabetes, and ratio of ALT:AST. The FSI identified patients with hepatic steatosis with a c-statistic value of 0.845. When it was applied to the third National Health and Nutrition Examination Survey cohort, the FSI identified patients with steatosis with a c-statistic value of 0.760 and was well-calibrated.
Conclusions: In an analysis of the Framingham Third Generation Cohort, we found the ratio of ALT:AST to identify people with hepatic steatosis more accurately than either ALT or AST alone. We used data from this cohort to develop and validate the FSI, which identifies patients with steatosis with a c-statistic value of about 0.8.
Keywords: Diagnostic; Diagnostic Score; Liver Fat; NAFLD.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Alimentary pharmacology & therapeutics. 2011;34(3):274–85. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55(6):2005–23. - PubMed
-
- Clark J. The prevalence and etiology of elevated aminotransferase levels in the United States. The American Journal of Gastroenterology. 2003;98(5):960–7. - PubMed
-
- Westerbacka J, Corner A, Tiikkainen M, et al. Women and men have similar amounts of liver and intra-abdominal fat, despite more subcutaneous fat in women: implications for sex differences in markers of cardiovascular risk. Diabetologia. 2004;47(8):1360–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
