

Viscoat Assisted Inverted Internal Limiting Membrane Flap Technique for Large Macular Holes Associated with High Myopia
- PMID: 27047686
- PMCID: PMC4800100
- DOI: 10.1155/2016/8283062
Viscoat Assisted Inverted Internal Limiting Membrane Flap Technique for Large Macular Holes Associated with High Myopia
Abstract
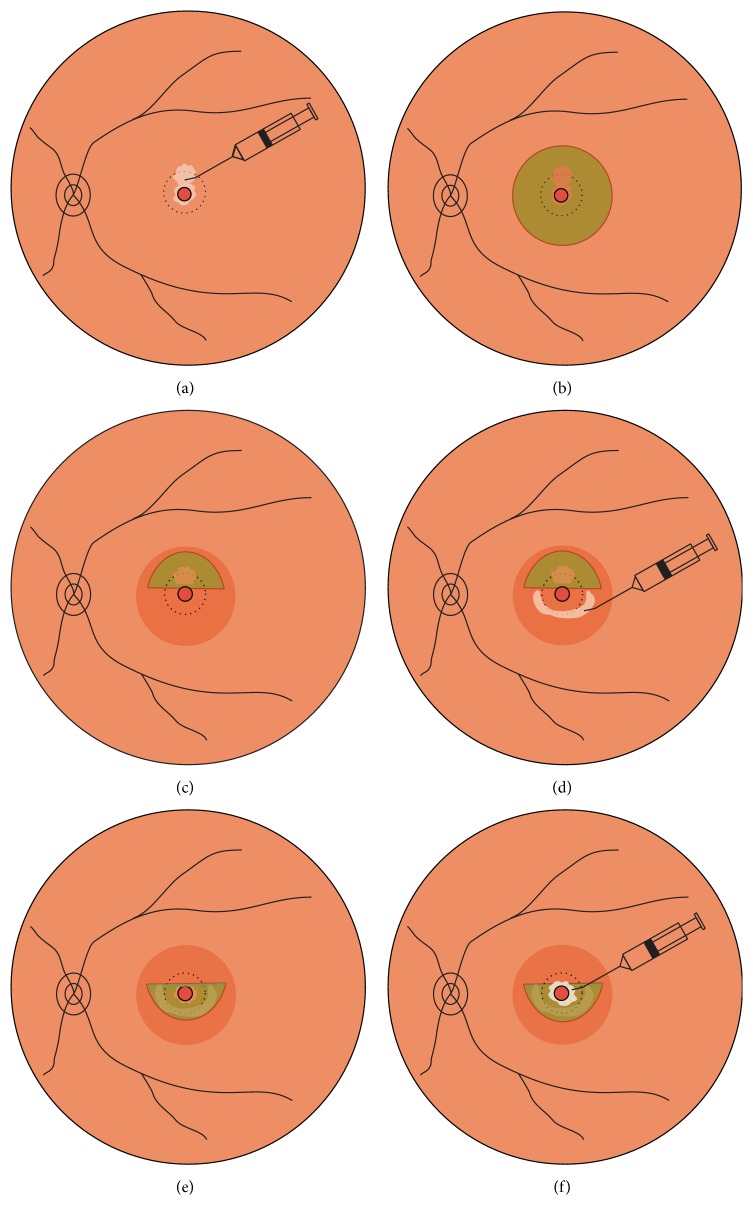
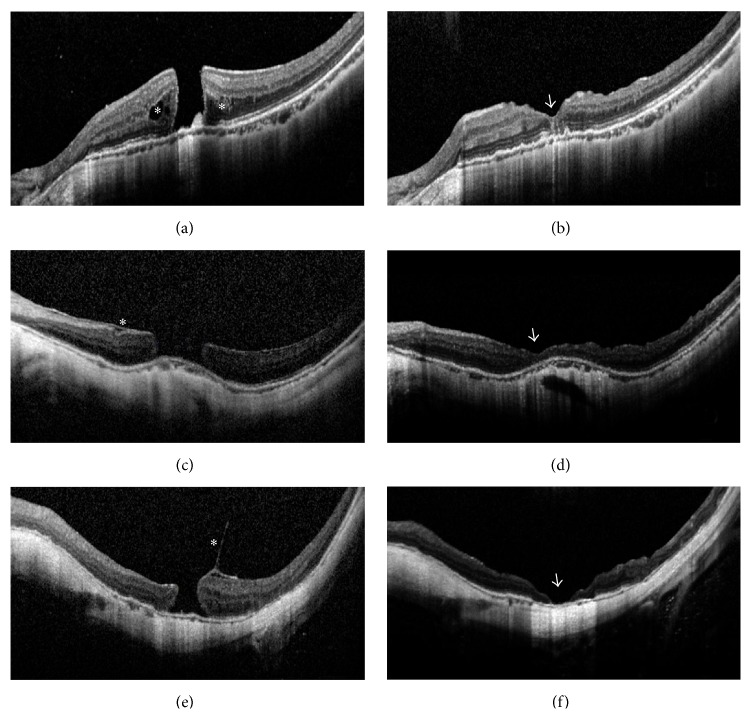
Purpose. To investigate the surgical outcomes of Viscoat® assisted inverted internal limiting membrane (ILM) flap technique for large macular holes (MHs) associated with high myopia. Design. Prospective, interventional case series. Methods. Fifteen eyes of 15 patients with high myopia underwent vitrectomy and Viscoat assisted inverted ILM flap technique to treat MH without RD. Patients were followed up over 6 months. The main outcome measures were MH closure evaluated by optical coherence tomography (OCT) and best-corrected visual acuities (BCVAs). Result. MH closure was observed in all eyes (100%) following the initial surgery. Type 1 closure was observed in 13 eyes (86.7%); type 2 closure was observed in the remaining 2 eyes (13.3%). Compared to the preoperative baseline, the mean BCVA (logarithm of the minimum angle of resolution) improved significantly at 3 months and 6 months after surgery (P = 0.025, 0.019, resp.). The final BCVA improved in 10 eyes (66.7%), remained unchanged in 3 eyes (20.0%), and worsened in 2 eyes (13.3%). Conclusion. Vitrectomy combined with Viscoat assisted inverted ILM flap technique is an effective treatment for large MHs in highly myopic eyes. It may increase the success rate of the initial surgery and enhance the anatomical and functional outcomes.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
