

Overestimate of Fibrosis by FIBROSpect® II in African Americans Complicates the Management of their Chronic Hepatitis C
- PMID: 27047767
- PMCID: PMC4807138
- DOI: 10.14218/JCTH.2015.00053
Overestimate of Fibrosis by FIBROSpect® II in African Americans Complicates the Management of their Chronic Hepatitis C
Abstract
Background: Evaluation of advanced fibrosis in patients with hepatitis C virus (HCV) infection is used to facilitate decisions on treatment strategy and to initiate additional screening measures. Unfortunately, most studies have predominately Caucasian (Cau) patients and may not be as relevant for African Americans (AA).
Aims: This study specifically addresses the issue of defining minimal vs. significant fibrosis in African Americans (AA) with chronic hepatitis C (CHC) using noninvasive assays.
Methods: All patients (n = 319) seen between 1 January 2008 and 30 June 2013 for whom a FibroSpect II® (FSII) assay was performed and had data for calculation of aspartate aminotransferase (AST) platelet ratio index (APRI) and Fibrosis-4 (FIB-4) were identified using the medical records.
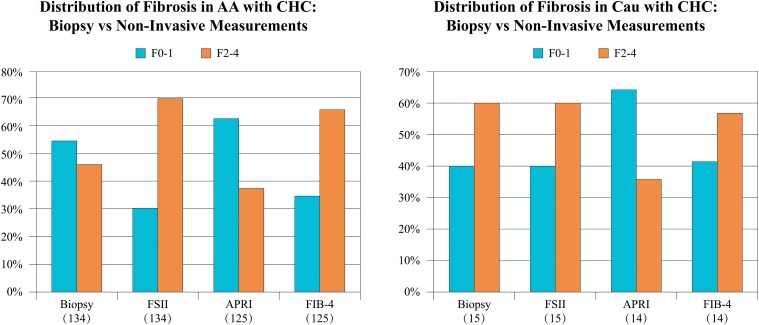
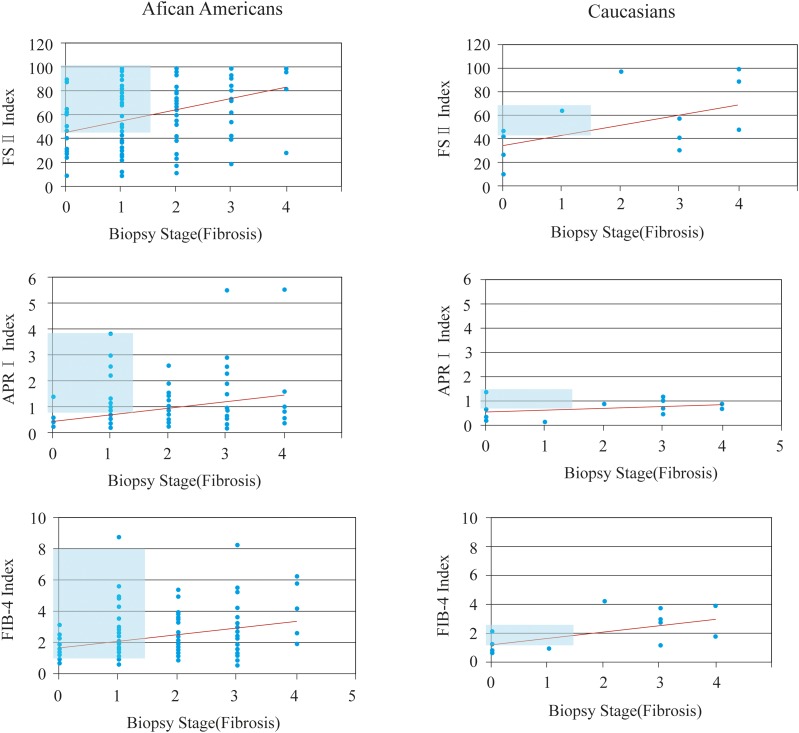
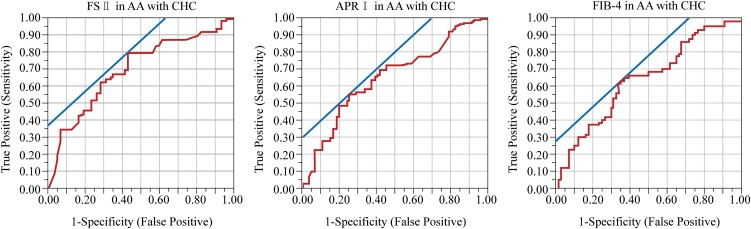
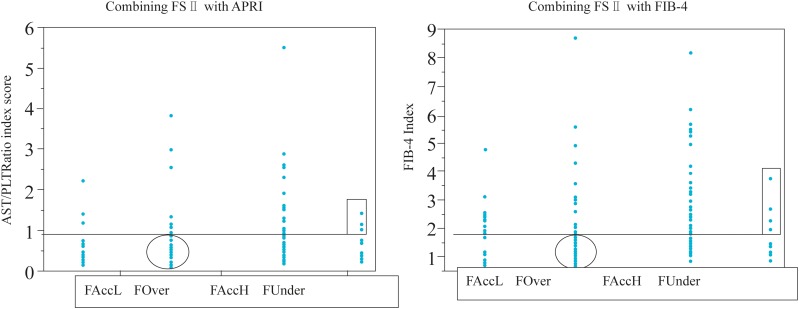
Results: When liver biopsy score and FSII assay results for the AA patients with CHC were compared, 31% of AA had advanced FSII fibrosis scores (F2-F4) despite a biopsy score of F0-F1. In contrast, 10% of Cau over-scored. The AA false positive rate was 14% for APRI and 34% for FIB-4. Combining FSII with either APRI (7% false positive) or FIB-4 (10% false positive) improved the false positive rate in AA to 7% (FSII + APRI) and 10% (FSII + FIB-4) but reduced the sensitivity for significant fibrosis.
Conclusions: The FSII assay overestimates fibrosis in AA and should be used with caution since these patients may not have significant fibrosis. If the APRI or FIB-4 assay is combined with the FSII assay, minimal fibrosis in AA can be defined without subjecting the patients to a subsequent biopsy.
Keywords: African Americans; Fibrosis; Fibrospect; Hepatitis c.
Conflict of interest statement
Figures
Similar articles
-
The APRI may be enhanced by the use of the FIBROSpect II in the estimation of fibrosis in chronic hepatitis C.Clin Chim Acta. 2007 Jun;381(2):119-23. doi: 10.1016/j.cca.2007.02.046. Epub 2007 Mar 19. Clin Chim Acta. 2007. PMID: 17442291
-
Correlation of FIBROSpect II with histologic and morphometric evaluation of liver fibrosis in chronic hepatitis C.Clin Gastroenterol Hepatol. 2008 Feb;6(2):242-7. doi: 10.1016/j.cgh.2007.11.009. Epub 2008 Jan 9. Clin Gastroenterol Hepatol. 2008. PMID: 18187364
-
Serum Fibrosis Marker Panels FIB-4 Index and Aspartate Aminotransferase (AST)-to-Platelet Ratio Index (APRI) Are Equivalent to AST Alone at Predicting Liver Fibrosis in a Cohort of 1731 Patients Infected with Hepatitis C Virus.J Appl Lab Med. 2017 Jul 1;2(1):76-85. doi: 10.1373/jalm.2016.022509. J Appl Lab Med. 2017. PMID: 33636957
-
Fibrosis index based on four factors better predicts advanced fibrosis or cirrhosis than aspartate aminotransferase/platelet ratio index in chronic hepatitis C patients.J Formos Med Assoc. 2015 Oct;114(10):923-8. doi: 10.1016/j.jfma.2015.07.004. Epub 2015 Aug 13. J Formos Med Assoc. 2015. PMID: 26279173
-
Diagnostic value of combined serum biomarkers for the evaluation of liver fibrosis in chronic hepatitis C infection: A multicenter, noninterventional, observational study.Turk J Gastroenterol. 2018 Jul;29(4):464-472. doi: 10.5152/tjg.2018.16597. Turk J Gastroenterol. 2018. PMID: 30249562 Free PMC article.
References
-
- Shiffman ML, Benhamou Y. Patients with HCV and F1 and F2 fibrosis stage: treat now or wait? Liver Int. 2013;33:105–110. doi: 10.1111/liv.12066. - PubMed
-
- Manning DS, Afdhal NH. Diagnosis and quantitation of fibrosis. Gastroenterology. 2008;134:1670–1681. doi: 10.1053/j.gastro.2008.03.001. - PubMed
-
- Baran B, Gulluoglu M, Soyer OM, Ormeci AC, Gokturk S, Evirgen SF, et al. Treatment failure may lead to accelerated fibrosis progression in patients with chronic hepatitis C. J Viral Hepat. 2014;21:111–120. doi: 10.1111/jvh.12127. - PubMed
-
- Morishita N, Hiramatsu N, Oze T, Harada N, Yamada R, Miyazaki M, et al. Liver stiffness measurement by acoustic radiation force impulse is useful in predicting the presence of esophageal varices or high-risk esophageal varices among patients with HCV-related cirrhosis. J Gastroenterol. 2014;49:1175–1182. doi: 10.1007/s00535-013-0877-z. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous